

Timing of Medicaid Enrollment, Late-Stage Breast Cancer Diagnosis, Treatment Delays, and Mortality
- PMID: 35583139
- PMCID: PMC9113434
- DOI: 10.1093/jncics/pkac031
Timing of Medicaid Enrollment, Late-Stage Breast Cancer Diagnosis, Treatment Delays, and Mortality
Abstract
Background: Disrupted and delayed Medicaid coverage has been consistently associated with lower rates of cancer screening and early-stage cancer diagnosis compared with continuous coverage. However, the relationships between Medicaid coverage timing, breast cancer treatment delays, and survival are less clear.
Methods: Using the linked Missouri Cancer Registry-Medicaid claims data, we identified 4583 women diagnosed with breast cancer between 2007 and 2016. We used logistic regression to estimate odds ratios (ORs) of late-stage diagnosis and treatment delays for prediagnosis (>30 days, >90 days, and >1 year before diagnosis) vs peridiagnosis enrollment. Cox proportional hazards models were used to estimate the hazard ratio (HR) of breast cancer-specific mortality for pre- vs postdiagnosis enrollment.
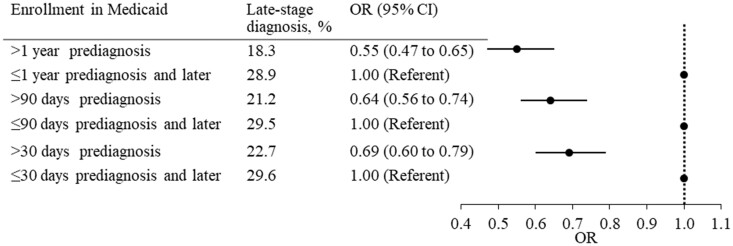
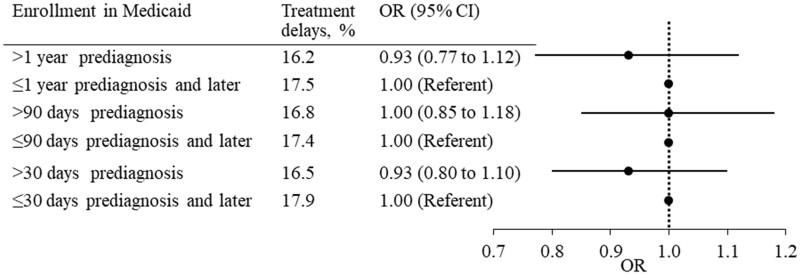
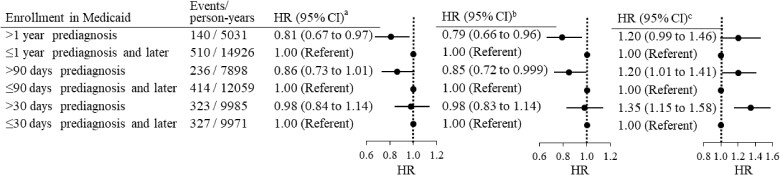
Results: Patients enrolled in Medicaid more than 30 days before diagnosis were less likely to be diagnosed at a late stage compared with those enrolled in Medicaid peridiagnosis (OR = 0.69, 95% confidence interval [CI] = 0.60 to 0.79). This result persisted using enrollment 90-day (OR = 0.64, 95% CI = 0.56 to 0.74) and 1-year thresholds (OR = 0.55, 95% CI = 0.47 to 0.65). We did not observe a difference in the likelihood of treatment delays between the 2 groups. After adjustment for sociodemographic factors, there was no statistically significant difference in the risk of breast cancer mortality for patients enrolled more than 30 days prediagnosis relative to patients enrolled peridiagnosis (HR = 0.98, 95% CI = 0.83 to 1.14), but a lower risk was observed for patients enrolled prediagnosis when using 90 days (HR = 0.85, 95% CI = 0.72 to 0.999) or 1 year (HR = 0.79, 95% CI = 0.66 to 0.96) as the threshold.
Conclusions: Women with breast cancer who enroll in Medicaid earlier may benefit from earlier diagnoses, but only longer-term enrollment may have survival benefits.
© The Author(s) 2022. Published by Oxford University Press.
Figures
References
-
- Wilson J, Sule AA.. Disparity in early detection of breast cancer. In: StatPearls.com. Treasure Island (FL: ): StatPearls Publishing; 2020. http://www.ncbi.nlm.nih.gov/books/NBK564311/. Accessed December 5, 2021. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical