

IgA Serological Response for the Diagnosis of Mycobacterium abscessus Infections in Patients with Cystic Fibrosis
- PMID: 35583329
- PMCID: PMC9241595
- DOI: 10.1128/spectrum.00192-22
IgA Serological Response for the Diagnosis of Mycobacterium abscessus Infections in Patients with Cystic Fibrosis
Abstract
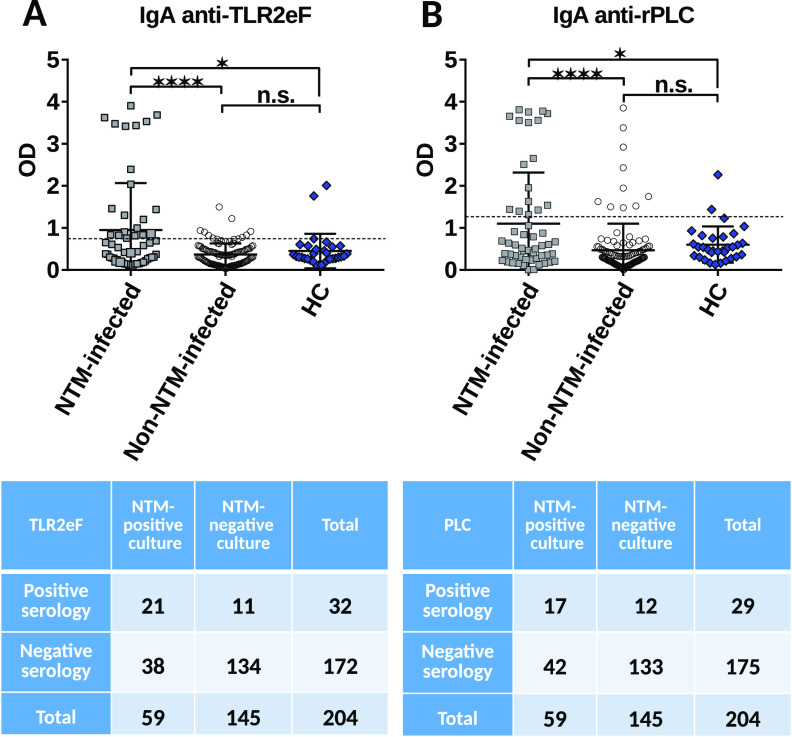
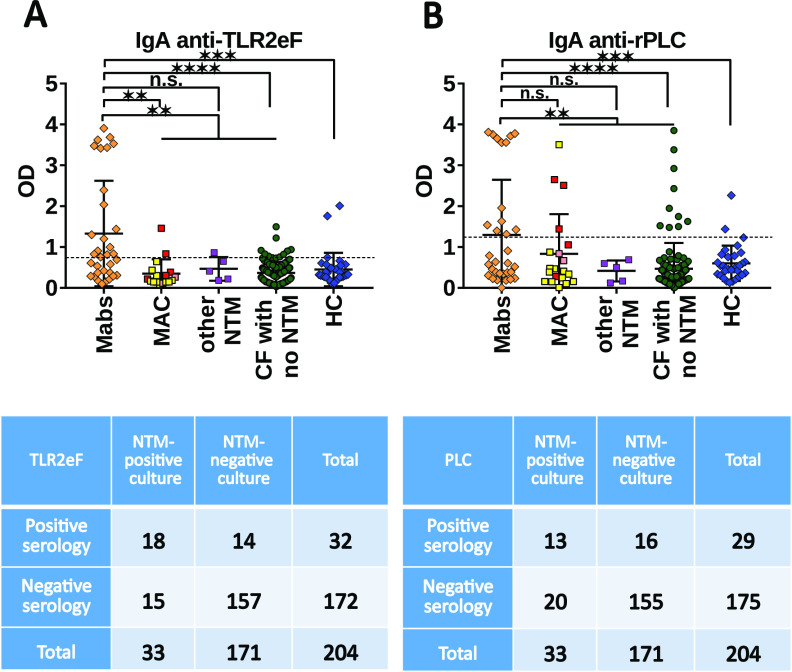
The immunoglobulin A (IgA) status of cystic fibrosis (CF) patients, presenting with or without a non-tuberculous mycobacterial (NTM) infection, has to date not been fully elucidated toward two antigenic preparations previously described. We have chosen to determine the clinical values of an IgA ELISA for the diagnosis of NTM and/or Mycobacterium abscessus infections in CF patients. One hundred and 73 sera from CF patients, comprising 33 patients with M. abscessus positive cultures, and 31 non-CF healthy controls were assessed. IgA levels were evaluated by indirect ELISAs using a surface antigenic extract named TLR2eF for TLR2 positive extract and a recombinant protein, the phospholipase C (rMAB_0555 or rPLC). These assays revealed a sensitivity of 52.6% (95% CI = 35.8% to 69%) and 42.1% (95% CI = 26.3% to 59.2%) using TLR2eF and rPLC, respectively, and respective specificities of 92.6% (95% CI = 87.5% to 96.1%) and 92% (95% CI = 86.7% to 95.7%) for samples culture positive for M. abscessus. Overall sensitivity and specificity of 66.7% and 85.4%, respectively, were calculated for IgA detection in M. abscessus-culture positive CF patients, when we combine the results of the two used antigens, thus demonstrating the efficiency in detection of positive cases for these two antigens with IgA isotype. CF patients with a positive culture for M. abscessus had the highest IgA titers against TLR2eF and rPLC. The diagnosis of NTM infections, including those due to M. abscessus, can be improved by the addition of an IgA serological assay, especially when cultures, for example, are negative. Based on these promising results, a serological follow-up of a larger number of patients should be performed to determine if the IgA response may be correlated with an active/acute infection state or a very recent infection. IMPORTANCE Mycobacterium abscessus is currently the most frequently isolated rapid growing mycobacterium in human pathology and the major one involved in lung infections. It has recently emerged as responsible for severe pulmonary infections in patients with cystic fibrosis (CF) or those who have undergone lung transplantation. In addition, it represents the most antibiotic resistant mycobacterial species. However, despite its increasing clinical importance, very little is known about the use of M. abscessus parietal compounds and the host response. This has led to the development of serological tests to measure the antibody response in infected patients, and potentially to link this to the culture of respiratory samples. Herein, we describe an important analysis of the serological IgA response from CF patients, and we demonstrate the full diagnostic usefulness of this assay in the diagnosis of NTM infections, and more particularly M. abscessus, in CF patients.
Keywords: ELISA; IgA; cystic fibrosis; non-tuberculous mycobacteria; serodiagnosis; serology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Serological biomarkers for the diagnosis of Mycobacterium abscessus infections in cystic fibrosis patients.J Cyst Fibros. 2022 Mar;21(2):353-360. doi: 10.1016/j.jcf.2021.08.019. Epub 2021 Sep 10. J Cyst Fibros. 2022. PMID: 34511392
-
Specificity of Immunoglobulin Response to Nontuberculous Mycobacteria Infection in People with Cystic Fibrosis.Microbiol Spectr. 2022 Aug 31;10(4):e0187422. doi: 10.1128/spectrum.01874-22. Epub 2022 Jul 6. Microbiol Spectr. 2022. PMID: 35863022 Free PMC article.
-
Epidemiology of Pulmonary Nontuberculous Mycobacterial Sputum Positivity in Patients with Cystic Fibrosis in the United States, 2010-2014.Ann Am Thorac Soc. 2018 Jul;15(7):817-826. doi: 10.1513/AnnalsATS.201709-727OC. Ann Am Thorac Soc. 2018. PMID: 29897781 Free PMC article.
-
Pulmonary nontuberculous mycobacterial infections among women with cystic fibrosis and non-cystic fibrosis bronchiectasis.Ther Adv Respir Dis. 2025 Jan-Dec;19:17534666251323181. doi: 10.1177/17534666251323181. Epub 2025 Mar 12. Ther Adv Respir Dis. 2025. PMID: 40071337 Free PMC article. Review.
-
Nontuberculous mycobacterial infections in cystic fibrosis.Clin Chest Med. 2015 Mar;36(1):101-15. doi: 10.1016/j.ccm.2014.11.003. Clin Chest Med. 2015. PMID: 25676523 Review.
Cited by
-
The roles of neutrophils in non-tuberculous mycobacterial pulmonary disease.Ann Clin Microbiol Antimicrob. 2023 Feb 18;22(1):14. doi: 10.1186/s12941-023-00562-6. Ann Clin Microbiol Antimicrob. 2023. PMID: 36800956 Free PMC article. Review.
-
A glycosylated lipooctapeptide promotes uptake and growth of Mycobacterium abscessus in the host.Nat Commun. 2025 Apr 8;16(1):3326. doi: 10.1038/s41467-025-58455-5. Nat Commun. 2025. PMID: 40199904 Free PMC article.
References
-
- Jalkanen P, Pasternack A, Maljanen S, Melén K, Kolehmainen P, Huttunen M, Lundberg R, Tripathi L, Khan H, Ritvos MA, Naves R, Haveri A, Österlund P, Kuivanen S, Jääskeläinen AJ, Kurkela S, Lappalainen M, Rantasärkkä K, Vuorinen T, Hytönen J, Waris M, Tauriainen S, Ritvos O, Kakkola L, Julkunen I. 2021. A combination of N and S antigens with IgA and IgG measurement strengthens the accuracy of SARS-CoV-2 serodiagnostics. J Infect Dis 224:218–228. doi:10.1093/infdis/jiab222. - DOI - PMC - PubMed
-
- Jamiruddin MR, Haq MA, Tomizawa K, Kobatake E, Mie M, Ahmed S, Khandker SS, Ali T, Jahan N, Oishee MJ, Khondoker MU, Sil BK, Haque M, Adnan N. 2021. Longitudinal antibody dynamics against structural proteins of SARS-CoV-2 in three COVID-19 patients shows concurrent development of IgA, IgM, and IgG. J Inflamm Res 14:2497–2506. doi:10.2147/JIR.S313188. - DOI - PMC - PubMed
-
- Fumimoto R, Otsuka N, Kamiya H, Sunagawa T, Tanaka-Taya K, Kamachi K, Shibayama K. 2019. Seroprevalence of IgA and IgM antibodies to Bordetella pertussis in healthy Japanese donors: assessment for the serological diagnosis of pertussis. PLoS One 14:e0219255. doi:10.1371/journal.pone.0219255. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
