

Intraductal tubulopapillary neoplasm (ITPN) of the pancreas: a distinct entity among pancreatic tumors
- PMID: 35583805
- PMCID: PMC9544156
- DOI: 10.1111/his.14698
Intraductal tubulopapillary neoplasm (ITPN) of the pancreas: a distinct entity among pancreatic tumors
Abstract
Aims: Intraductal tubulopapillary neoplasm (ITPN) of the pancreas is a recently recognized pancreatic tumor entity. Here we aimed to determine the most important features with a systematic review coupled with an integrated statistical approach.
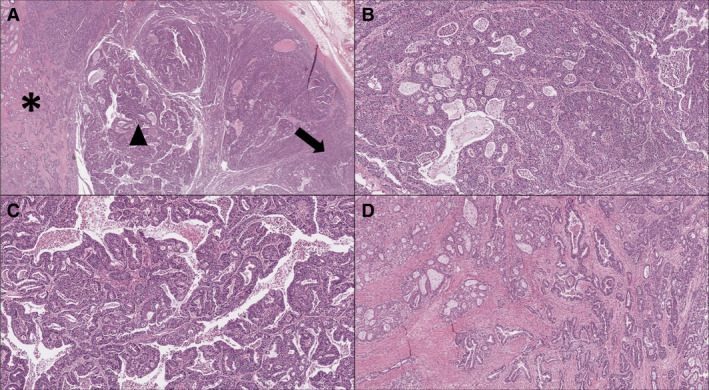
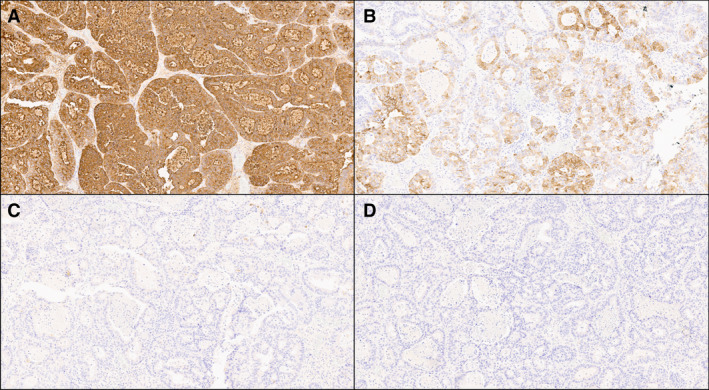
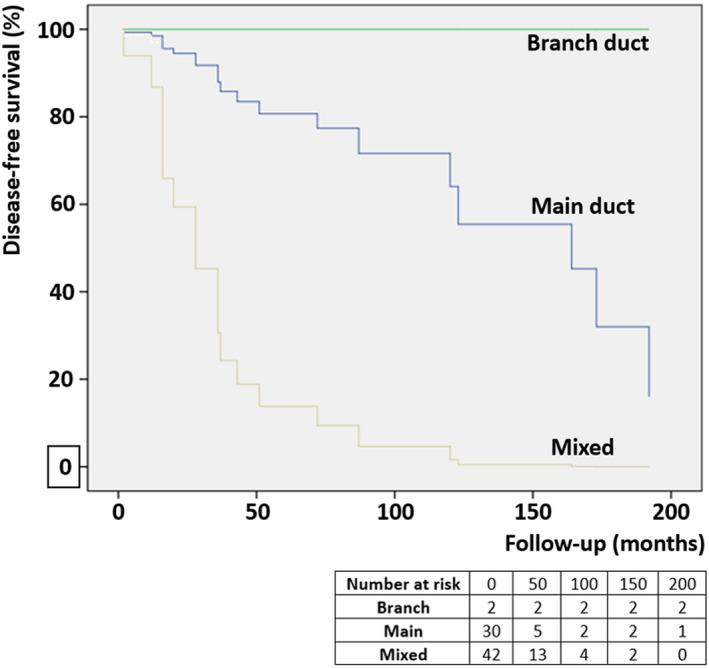
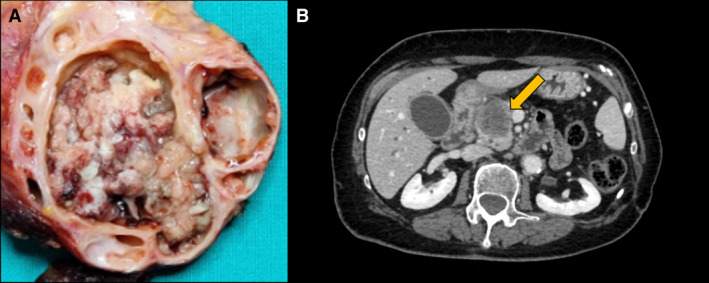
Methods and results: PubMed, SCOPUS, and Embase were searched for studies reporting data on pancreatic ITPN. The clinicopathological, immunohistochemical, and molecular data were summarized. Then a comprehensive survival analysis and a comparative analysis of the molecular alterations of ITPN with those of pancreatic ductal adenocarcinoma (PDAC) and intraductal papillary mucinous neoplasm (IPMN) from reference cohorts (including the International Cancer Genome Consortium- ICGC dataset and The Cancer Genome Atlas, TCGA program) were conducted. The core findings of 128 patients were as follows: (i) Clinicopathological parameters: pancreatic head is the most common site; presence of an associated adenocarcinoma was reported in 60% of cases, but with rare nodal metastasis. (ii) Immunohistochemistry: MUC1 (>90%) and MUC6 (70%) were the most frequently expressed mucins. ITPN lacked the intestinal marker MUC2; unlike IPMN, it did not express MUC5AC. (iii) Molecular landscape: Compared with PDAC/IPMN, the classic pancreatic drivers KRAS, TP53, CDKN2A, SMAD4, GNAS, and RNF43 were less altered in ITPN (P < 0.001), whereas MCL amplifications, FGFR2 fusions, and PI3KCA mutations were commonly altered (P < 0.001). (iv) Survival analysis: ITPN with a "pure" branch duct involvement showed the lowest risk of recurrence.
Conclusion: ITPN is a distinct pancreatic neoplasm with specific clinicopathological and molecular characteristics. Its recognition is fundamental for its clinical/prognostic implications and for the enrichment of potential targets for precision oncology.
Keywords: IPMN; ITPN; PDAC; intraductal; pancreas; pancreatic ductal adenocarcinoma; tubulopapillary.
© 2022 The Authors. Histopathology published by John Wiley & Sons Ltd.
Conflict of interest statement
There are no conflicts of interest to report.
Figures
Similar articles
-
Clinicopathological features and surgical outcomes of intraductal tubulopapillary neoplasm of the pancreas: a systematic review.Langenbecks Arch Surg. 2016 Jun;401(4):439-47. doi: 10.1007/s00423-016-1391-6. Epub 2016 Mar 21. Langenbecks Arch Surg. 2016. PMID: 27001682
-
Systematic review of resectable intraductal tubulopapillary neoplasm with special reference to recurrence patterns.Surg Today. 2022 Apr;52(4):532-541. doi: 10.1007/s00595-021-02324-3. Epub 2021 Jul 1. Surg Today. 2022. PMID: 34196805
-
Mucinous cystic neoplasms and simple mucinous cysts are two distinct precursors of pancreatic cancer: clinicopathological, genomic, and transcriptomic characterization.J Pathol. 2025 Aug;266(4-5):421-434. doi: 10.1002/path.6437. Epub 2025 May 15. J Pathol. 2025. PMID: 40371932 Free PMC article.
-
Important radiological and clinicopathological risk factors for the recurrence of intraductal papillary mucinous neoplasms after surgical resection.Eur Radiol. 2025 Aug;35(8):5004-5016. doi: 10.1007/s00330-025-11431-5. Epub 2025 Feb 19. Eur Radiol. 2025. PMID: 39971792 Free PMC article.
-
[A rare case of intraductal tumor of the pancreas in which an intraductal tubulopapillary neoplasm was mixed with a widely spreading gastric-type intraductal papillary-mucinous neoplasm].Nihon Shokakibyo Gakkai Zasshi. 2024;121(5):415-424. doi: 10.11405/nisshoshi.121.415. Nihon Shokakibyo Gakkai Zasshi. 2024. PMID: 38735750 Japanese.
Cited by
-
A case of pancreatic ductal adenocarcinoma growing within the pancreatic duct mimicking an intraductal tubulopapillary neoplasm.Clin J Gastroenterol. 2025 Apr;18(2):376-382. doi: 10.1007/s12328-025-02098-y. Epub 2025 Feb 5. Clin J Gastroenterol. 2025. PMID: 39910028 Free PMC article.
-
Neoplastic premalignant pancreatobiliary lesions: current update on the spectrum of lesions and their imaging appearances.Abdom Radiol (NY). 2025 Aug;50(8):3647-3661. doi: 10.1007/s00261-024-04795-7. Epub 2025 Jan 13. Abdom Radiol (NY). 2025. PMID: 39804368 Review.
-
Modern aspects of the management of pancreatic intraductal papillary mucinous neoplasms: a narrative review.Rom J Morphol Embryol. 2022 Jul-Sep;63(3):491-502. doi: 10.47162/RJME.63.3.03. Rom J Morphol Embryol. 2022. PMID: 36588487 Free PMC article. Review.
-
Integrative characterization of intraductal tubulopapillary neoplasm (ITPN) of the pancreas and associated invasive adenocarcinoma.Mod Pathol. 2022 Dec;35(12):1929-1943. doi: 10.1038/s41379-022-01143-2. Epub 2022 Sep 2. Mod Pathol. 2022. PMID: 36056133 Free PMC article.
-
Improving the prognosis of pancreatic cancer: insights from epidemiology, genomic alterations, and therapeutic challenges.Front Med. 2023 Dec;17(6):1135-1169. doi: 10.1007/s11684-023-1050-6. Epub 2023 Dec 27. Front Med. 2023. PMID: 38151666 Review.
References
-
- Sung H, Ferlay J, Siegel RL et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021; 71; 209–249. - PubMed
-
- Mizrahi JD, Surana R, Valle JW et al. Pancreatic cancer. Lancet 2020; 395; 2008–2020. - PubMed
-
- Singhi AD, Wood LD. Early detection of pancreatic cancer using DNA‐based molecular approaches. Nat. Rev. Gastroenterol. Hepatol. 2021; 18; 457–468. - PubMed
-
- Kim JY, Hong S‐M. Precursor lesions of pancreatic cancer. Oncol. Res. Treat. 2018; 41; 603–610. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
