

Utility of Biomarkers for Sepsis-Associated Acute Kidney Injury Staging
- PMID: 35583867
- PMCID: PMC9118077
- DOI: 10.1001/jamanetworkopen.2022.12709
Utility of Biomarkers for Sepsis-Associated Acute Kidney Injury Staging
Abstract
Importance: The 23rd Acute Disease Quality Initiative (ADQI-23) consensus conference proposed a framework to integrate biomarkers into the staging of acute kidney injury (AKI). It is unknown whether tissue inhibitor of metalloproteinases 2 (TIMP-2) and insulinlike growth factor binding protein 7 (IGFBP7) could be used for staging.
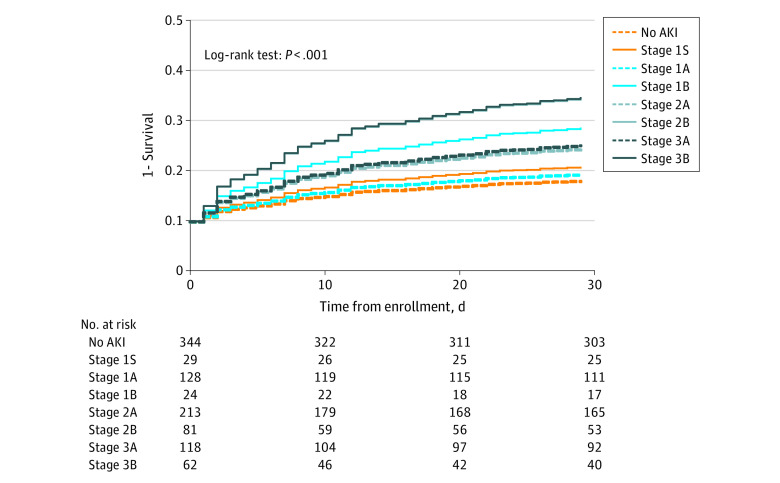
Objective: To test whether higher levels of urinary [TIMP-2] × [IGFBP7] are associated with lower survival among patients with the same functional stage of AKI.
Design, setting, and participants: This cohort study was performed using data from the Protocolized Care for Early Septic Shock (ProCESS) trial, which enrolled critically ill patients with septic shock who presented at academic and community emergency departments and intensive care units in the US from March 2008 to May 2013. Patients with end-stage kidney disease, a reference serum creatinine level of 4 mg/dL or greater (to convert to μmol/L, multiply by 76.25), or missing data on serum creatinine levels or urinary levels of [TIMP-2] × [IGFBP7] were excluded. Data were analyzed from October 2020 to October 2021.
Exposures: The presence of AKI, assessed using Kidney Disease: Improving Global Outcomes criteria within 24 hours after enrollment and the highest AKI stage as well as urinary [TIMP-2] × [IGFBP7] level at 6 hours after enrollment. A previously reported high-specificity cutoff level for [TIMP-2] × [IGFBP7] of 2.0 (ng/mL)2/1000 was used to categorize patients (including those without functional criteria of AKI) according to the new staging system proposed by the ADQI-23 as biomarker negative (urinary [TIMP-2] × [IGFBP7] level ≤2.0 [ng/mL]2/1000) or biomarker positive ([TIMP-2] × [IGFBP7] >2.0 [ng/mL]2/1000).
Main outcomes and measures: Survival (assessed using Kaplan-Meier plots and the log-rank test) and mortality (assessed using relative risk [RR] 30 days after enrollment).
Results: The analysis included 999 patients with a median age of 61 years (IQR, 50-73 years); 554 (55.5%) were male. Biomarker-positive patients had lower survival and higher mortality at 30 days in the groups with AKI stage 1 (RR, 2.20; 95% CI, 1.02-4.72), stage 2 (RR, 1.53; 95% CI, 1.04-2.27), and stage 3 (RR, 1.61; 95% CI, 1.00-2.60). The associations were specific to patients with AKI. No difference in 30-day survival was found between biomarker-positive and biomarker-negative patients in the absence of functional criteria for AKI (RR, 1.16; 95% CI, 0.45-3.01).
Conclusions and relevance: The findings suggest that assessment of the cell-cycle arrest biomarkers TIMP-2 and IGFBP7 may augment AKI staging for patients with functional criteria for AKI.
Conflict of interest statement
Figures

References
-
- Kellum JA, Lameire N, Aspelin P, et al. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group: KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2(1):1-138.
-
- Kudose S, Hoshi M, Jain S, Gaut JP. Renal histopathologic findings associated with severity of clinical acute kidney injury. Am J Surg Pathol. 2018;42(5):625-635. - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Chronic Kidney Disease Work Group. KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1-150.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
