

Retreatment for hepatitis C virus direct acting antiviral therapy virological failure in primary and tertiary settings: the REACH-C cohort
- PMID: 35583922
- PMCID: PMC9542502
- DOI: 10.1111/jvh.13705
Retreatment for hepatitis C virus direct acting antiviral therapy virological failure in primary and tertiary settings: the REACH-C cohort
Abstract
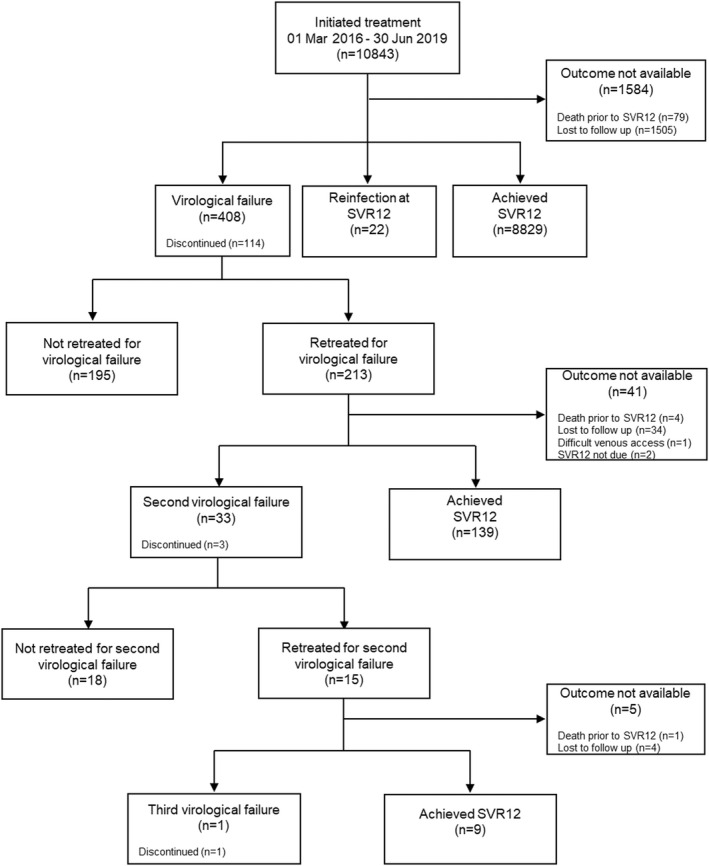
Virological failure occurs in a small proportion of people treated for hepatitis C virus (HCV) with direct-acting antiviral (DAA) therapies. This study assessed retreatment for virological failure in a large real-world cohort. REACH-C is an Australian observational study (n=10843) evaluating treatment outcomes of sequential DAA initiations across 33 health services between March 2016 to June 2019. Virological failure retreatment data were collected until October 2020. Of 408 people with virological failure (81% male; median age 53; 38% cirrhosis; 56% genotype 3), 213 (54%) were retreated once; 15 were retreated twice. A range of genotype specific and pangenotypic DAAs were used to retreat virological failure in primary (n=56) and tertiary (n=157) settings. Following sofosbuvir/velpatasvir/voxilaprevir availability in 2019, the proportion retreated in primary care increased from 21% to 40% and median time to retreatment initiation declined from 294 to 152 days. Per-protocol (PP) sustained virological response (SVR12) was similar for people retreated in primary and tertiary settings (80% vs 81%; p=1.000). In regression analysis, sofosbuvir/velpatasvir/voxilaprevir (vs. other regimens) significantly decreased likelihood of second virological failure (PP SVR12 88% vs. 77%; adjusted odds ratio [AOR] 0.29; 95%CI 0.11-0.81); cirrhosis increased likelihood (PP SVR12 69% vs. 91%; AOR 4.26; 95%CI 1.64-11.09). Indigenous Australians had lower likelihood of retreatment initiation (AOR 0.36; 95%CI 0.15-0.81). Treatment setting and prescriber type were not associated with retreatment initiation or outcome. Virological failure can be effectively retreated in primary care. Expanded access to simplified retreatment regimens through decentralised models may increase retreatment uptake and reduce HCV-related mortality.
Keywords: HCV; direct-acting antivirals; primary care; retreatment; virological failure.
This article is protected by copyright. All rights reserved.
Conflict of interest statement
GJD reports grants, personal fees and nonfinancial support from AbbVie, Gilead, Merck, Bristol‐Myers Squibb and Roche; grants and personal fees from Janssen; personal fees and nonfinancial support from Gilead Sciences; and personal fees from GlaxoSmithKline and Abbott Diagnostics. GVM reports grants from Gilead Sciences and grants from AbbVie. DI reports fees from Gilead, Merck, BMSand AbbVie. PR reports fees for educational talks from Gilead Sciences, Merck Sharp & Dohme and AbbVie and is on the advisory board for Merck Sharp & Dohme. AB reports sponsorship from Gilead to participate in online HCV medical educational modules. JDo reports grants to his institution for investigator initiated research and consulting fees from Gilead Sciences, Merck/MSD and AbbVie. JO reports speaker fees from Gilead and BMS. JC/JY/BH/JH/JDa/MM/PM report none.
Figures

References
-
- Hajarizadeh B, Grebely J, Dore GJ. Epidemiology and natural history of HCV infection. Nat Rev Gastroenterol Hepatol. 2013;10(9):553‐562. - PubMed
-
- Dore GJ, Martinello M, Alavi M, Grebely J. Global elimination of hepatitis C virus by 2030: why not? Nat Med. 2020;26(2):157‐160. - PubMed
-
- Razavi H, Sanchez Gonzalez Y, Yuen C, Cornberg M. Global timing of hepatitis C virus elimination in high‐income countries. Liver Int. 2020;40(3):522‐529. - PubMed
-
- Alavi M, Law MG, Valerio H, et al. Declining hepatitis C virus‐related liver disease burden in the direct‐acting antiviral therapy era in New South Wales, Australia. J Hepatol. 2019;71(2):281‐288. - PubMed
-
- Heard S, Iverson J, Geddes L, Maher L. Australian Needle and Syringe Program Survey 25 Year National Data Report 1995–2019; 2020.
LinkOut - more resources
Full Text Sources
Miscellaneous
