

A Risk Score to Detect Subclinical Rheumatoid Arthritis-Associated Interstitial Lung Disease
- PMID: 35583934
- PMCID: PMC9828082
- DOI: 10.1002/art.42162
A Risk Score to Detect Subclinical Rheumatoid Arthritis-Associated Interstitial Lung Disease
Abstract
Objective: Patients at high risk of rheumatoid arthritis-associated interstitial lung disease (RA-ILD) would benefit from being identified before the onset of respiratory symptoms; this can be done by screening patients with the use of chest high-resolution computed tomography (HRCT). Our objective was to develop and validate a risk score for patients who have subclinical RA-ILD.
Methods: Our study included a discovery population and a replication population from 2 prospective RA cohorts (ESPOIR and TRANSLATE2, respectively) without pulmonary symptoms who had received chest HRCT scans. All patients were genotyped for MUC5B rs35705950. After multiple logistic regression, a risk score based on independent risk factors for subclinical RA-ILD was developed in the discovery population and tested for validation in the replication population.
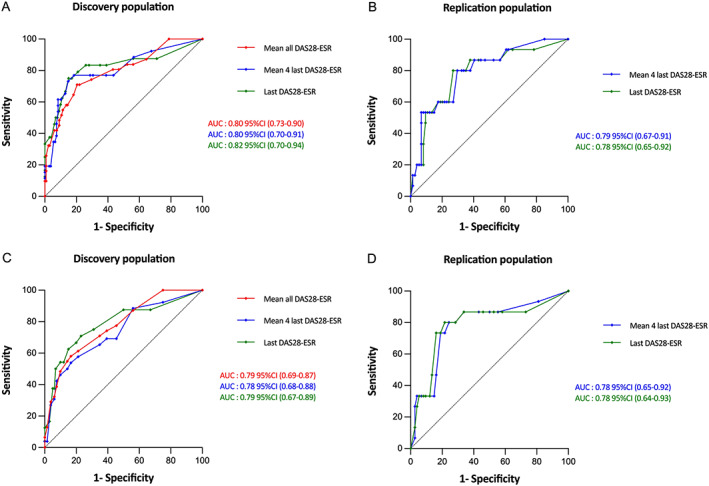
Results: The discovery population included 163 patients with RA, and the replication population included 89 patients with RA. The prevalence of subclinical RA-ILD was 19.0% and 16.9%, respectively. In the discovery population, independent risk factors for subclinical RA-ILD were presence of the MUC5B rs35705950 T allele (odds ratio [OR] 3.74 [95% confidence interval (95% CI) 1.37, 10.39]), male sex (OR 3.93 [95% CI 1.40, 11.39]), older age at RA onset (for each year, OR 1.10 [95% CI 1.04, 1.16]), and increased mean Disease Activity Score in 28 joints using the erythrocyte sedimentation rate (for each unit, OR 2.03 [95% CI 1.24, 3.42]). We developed and validated a derived risk score with receiver operating characteristic areas under the curve of 0.82 (95% CI 0.70-0.94) for the discovery population and 0.78 (95% CI 0.65-0.92) for the replication population. Excluding MUC5B rs35705950 from the model provided a lower goodness of fit (likelihood ratio test, P = 0.01).
Conclusion: We developed and validated a risk score that could help identify patients at high risk of subclinical RA-ILD. Our findings support an important contribution of MUC5B rs35705950 to subclinical RA-ILD risk.
© 2022 The Authors. Arthritis & Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures
Similar articles
-
MUC5B Promoter Variant and Rheumatoid Arthritis with Interstitial Lung Disease.N Engl J Med. 2018 Dec 6;379(23):2209-2219. doi: 10.1056/NEJMoa1801562. Epub 2018 Oct 20. N Engl J Med. 2018. PMID: 30345907 Free PMC article.
-
MUC5B promoter variant rs35705950 and rheumatoid arthritis associated interstitial lung disease survival and progression.Semin Arthritis Rheum. 2021 Oct;51(5):996-1004. doi: 10.1016/j.semarthrit.2021.07.002. Epub 2021 Jul 10. Semin Arthritis Rheum. 2021. PMID: 34411838
-
MUC5B promoter variant rs35705950, rare but significant susceptibility locus in rheumatoid arthritis-interstitial lung disease with usual interstitial pneumonia in Asian populations.RMD Open. 2022 Dec;8(2):e002790. doi: 10.1136/rmdopen-2022-002790. RMD Open. 2022. PMID: 36581384 Free PMC article.
-
The prevalence and risk factors of rheumatoid arthritis-associated interstitial lung disease: a systematic review and meta-analysis.Ann Med. 2024 Dec;56(1):2332406. doi: 10.1080/07853890.2024.2332406. Epub 2024 Mar 28. Ann Med. 2024. PMID: 38547537 Free PMC article.
-
Incidence, risk factors, and prognosis of acute exacerbation of rheumatoid arthritis-associated interstitial lung disease: a systematic review and meta-analysis.BMC Pulm Med. 2023 Jul 11;23(1):255. doi: 10.1186/s12890-023-02532-2. BMC Pulm Med. 2023. PMID: 37434169 Free PMC article.
Cited by
-
Polygenic risk scores for rheumatoid arthritis and idiopathic pulmonary fibrosis and associations with RA, interstitial lung abnormalities, and quantitative interstitial abnormalities among smokers.Semin Arthritis Rheum. 2025 Jun;72:152708. doi: 10.1016/j.semarthrit.2025.152708. Epub 2025 Mar 15. Semin Arthritis Rheum. 2025. PMID: 40090204
-
Fibrosing Progressive Interstitial Lung Disease in Rheumatoid Arthritis: A Multicentre Italian Study.J Clin Med. 2023 Nov 11;12(22):7041. doi: 10.3390/jcm12227041. J Clin Med. 2023. PMID: 38002655 Free PMC article.
-
Novel Therapeutic Approaches in Connective Tissue Disease-Associated Interstitial Lung Disease.Semin Respir Crit Care Med. 2024 Jun;45(3):435-448. doi: 10.1055/s-0044-1786155. Epub 2024 May 13. Semin Respir Crit Care Med. 2024. PMID: 38740369 Free PMC article. Review.
-
Screening for rheumatoid arthritis-associated interstitial lung disease-a Delphi-based consensus statement.Z Rheumatol. 2024 Mar;83(2):160-168. doi: 10.1007/s00393-023-01464-w. Epub 2024 Jan 19. Z Rheumatol. 2024. PMID: 38240817 Free PMC article.
-
ERS International Congress 2022: highlights from the Thoracic Surgery and Lung Transplantation Assembly.ERJ Open Res. 2023 Apr 17;9(2):00671-2022. doi: 10.1183/23120541.00671-2022. eCollection 2023 Mar. ERJ Open Res. 2023. PMID: 37077552 Free PMC article. Review.
References
-
- Koduri G, Norton S, Young A, et al. Interstitial lung disease has a poor prognosis in rheumatoid arthritis: results from an inception cohort. Rheumatology 2010;49:1483–9. - PubMed
-
- Gabbay E, Tarala R, Will R, et al. Interstitial lung disease in recent onset rheumatoid arthritis. Am J Respir Crit Care Med 1997;156:528–35. - PubMed
-
- Reynisdottir G, Karimi R, Joshua V, et al. Structural changes and antibody enrichment in the lungs are early features of anti–citrullinated protein antibody–positive rheumatoid arthritis. Arthritis Rheumatol 2014;66:31–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
