

Ionised and total hypocalcaemia in pregnancy: An analysis of prevalence and risk factors in a resource-limited setting, Cameroon
- PMID: 35584129
- PMCID: PMC9116680
- DOI: 10.1371/journal.pone.0268643
Ionised and total hypocalcaemia in pregnancy: An analysis of prevalence and risk factors in a resource-limited setting, Cameroon
Abstract
Introduction: Hypocalcaemia remains a prevalent laboratory finding in pregnancy, capable of inducing adverse maternofoetal outcomes. This study compares the prevalence of hypocalcaemia in apparently healthy pregnant women from the ionised, and total calcaemia viewpoints and further identifies factors associated with total crude and ionised hypocalcaemia in pregnancy.
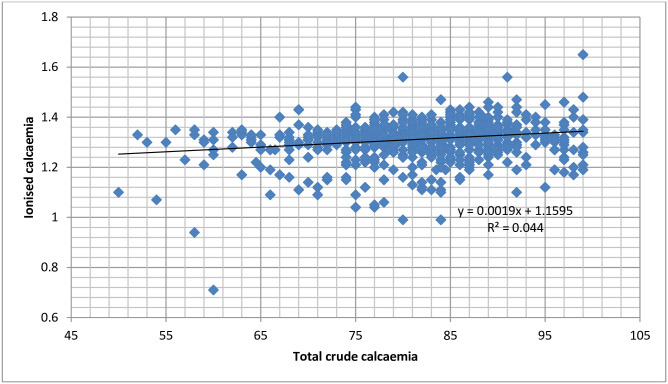
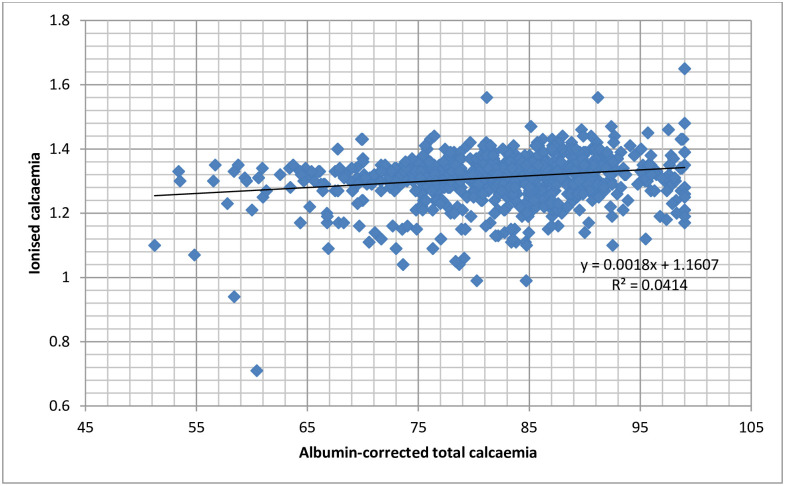
Methods: A hospital-based cross-sectional study was conducted between November 2020 and September 2021, targeting apparently healthy pregnant women received in late pregnancy in four maternities in the Nkongsamba Health District, Cameroon. Blood samples were collected and analysed for serum ionised calcium concentrations and pH (by ion-selective electrode potentiometry), and for total calcium and albumin concentration (by atomic absorption spectrophotometry). Sociodemographic, obstetric and nutritional data were collected using an interviewer-administered questionnaire.
Results: The average age of the 1074 participants included in the study was 28.20±6.08 years. The prevalence of total crude and total albumin-corrected hypocalcaemia in this study was 61.64 [58.69-64.50]% and 56.70 [53.72-59.64]%, respectively (p-value = 0.000). The prevalence of ionised hypocalcaemia was very low (2.89 [2.04-4.07]%) compared with the prevalence of total hypocalcaemia (p-value = 0.000). Monthly income below 100.000FCFA (179 USD) (AOR = 0.73, p-value = 0.024), taking more than 2 meals daily (AOR = 0.68, p-value = 0.006) and taking desserts (AOR = 0.73, p-value = 0.046) reduced the odds of total crude hypocalcaemia, while having banana/plantain and tubers as the content of their most consumed meal significantly increased the odds of total crude hypocalcaemia (AOR = 1.37, p-value = 0.012). Single women (AOR = 2.54, p-value = 0.021), with a higher education (AOR = 3.27, p-value = 0.017), who initiated antenatal care before 4 months (AOR = 2.47, p-value = 0.029), had their odds of ionised hypocalcaemia significantly increased. On the other hand, women below 30 years (AOR = 0.44, p-value = 0.039), with occupations other than housewife (AOR = 0.34, p-value = 0.027), and women who took desserts between meals (AOR = 0.45, p-value = 0.034) had their odds of ionised hypocalcaemia significantly reduced. Taking calcium supplements simultaneously with other supplements also significantly reduced the odds of total hypocalcaemia in pregnancy (OR = 0.69, p-value = 0.027).
Conclusion: Ionised hypocalcaemia in pregnancy is a rare finding. Only 2.89% of all apparently healthy pregnant women have ionised hypocalcaemia in late pregnancy, while 56.70% have total hypocalcaemia. Factors like the daily number of meals, taking of desserts, the content of the most consumed meal and monthly revenue significantly affect the prevalence of total hypocalcaemia in pregnancy. On the other hand, factors like age above 30 years, having a higher education, being single, having initiated antenatal care before 4 months of pregnancy, being a housewife and not taking desserts between meals have a significantly positive association with ionised hypocalcaemia.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Update of
-
Hypocalcaemia and calcium intake in pregnancy: A research protocol for critical analysis of risk factors, maternofoetal outcomes and evaluation of diagnostic methods in a third-category health facility, Cameroon.PLoS One. 2020 Nov 5;15(11):e0241812. doi: 10.1371/journal.pone.0241812. eCollection 2020. PLoS One. 2020. Update in: PLoS One. 2022 May 18;17(5):e0268643. doi: 10.1371/journal.pone.0268643. Update in: PLoS One. 2022 Aug 1;17(8):e0271525. doi: 10.1371/journal.pone.0271525. Update in: PLoS One. 2023 Oct 5;18(10):e0292303. doi: 10.1371/journal.pone.0292303. PMID: 33152011 Free PMC article. Updated.
References
-
- Benali AI, Demmouche A. Calcium Deficiency among Pregnant Women and their Newborns in Sidi Bel Abbes Region, Algeria. J Nutr Food Sci. 2014;04(06):4–7.
-
- Bako B, El-Nafaty AU, Mshelia DS, Gali RM, Isa B, Dungus MM. Prevalence and risk factors of hypocalcemia among pregnant and non-pregnant women in Maiduguri, Nigeria: A cross-sectional study. Niger J Clin Pract. 2021; - PubMed
-
- Eli S, Enyindah C, Orluwene C, Ikimalo J, Abam D. Prevalence of hypocalcaemia and maternal complications among antenatal clinic attendees at the university of Port Harcourt teaching hospital. Niger J Med. 2017;26(3):208.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
