

Cerebral perfusion in posterior reversible encephalopathy syndrome measured with arterial spin labeling MRI
- PMID: 35584601
- PMCID: PMC9119826
- DOI: 10.1016/j.nicl.2022.103017
Cerebral perfusion in posterior reversible encephalopathy syndrome measured with arterial spin labeling MRI
Abstract
Background and purpose: The pathophysiologic basis of posterior reversible encephalopathy syndrome (PRES) remains controversial. Hypertension (HTN)-induced autoregulatory failure with subsequent hyperperfusion is the leading hypothesis, whereas alternative theories suggest vasoconstriction-induced hypoperfusion as the underlying mechanism. Studies using contrast-based CT and MR perfusion imaging have yielded contradictory results supporting both ideas. This work represents one of the first applications of arterial spin labeling (ASL) to evaluate cerebral blood flow (CBF) changes in PRES.
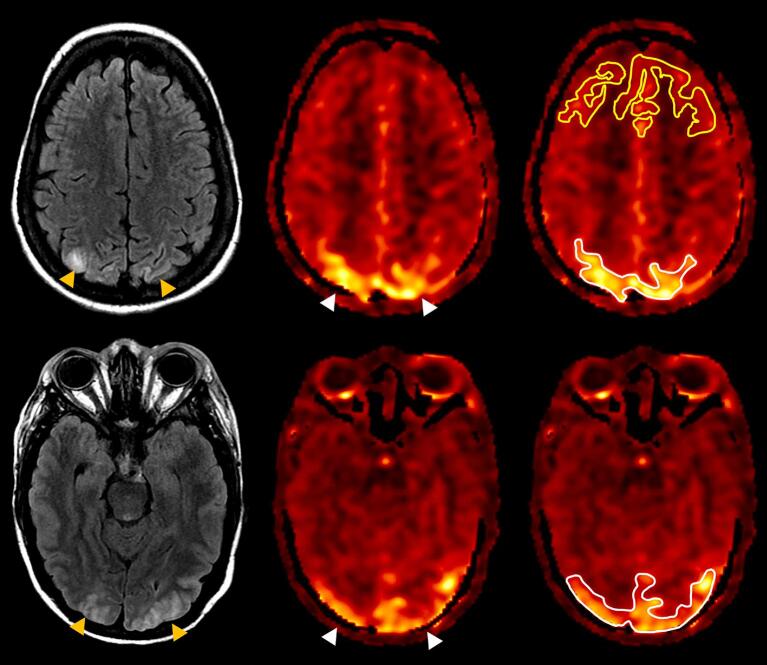
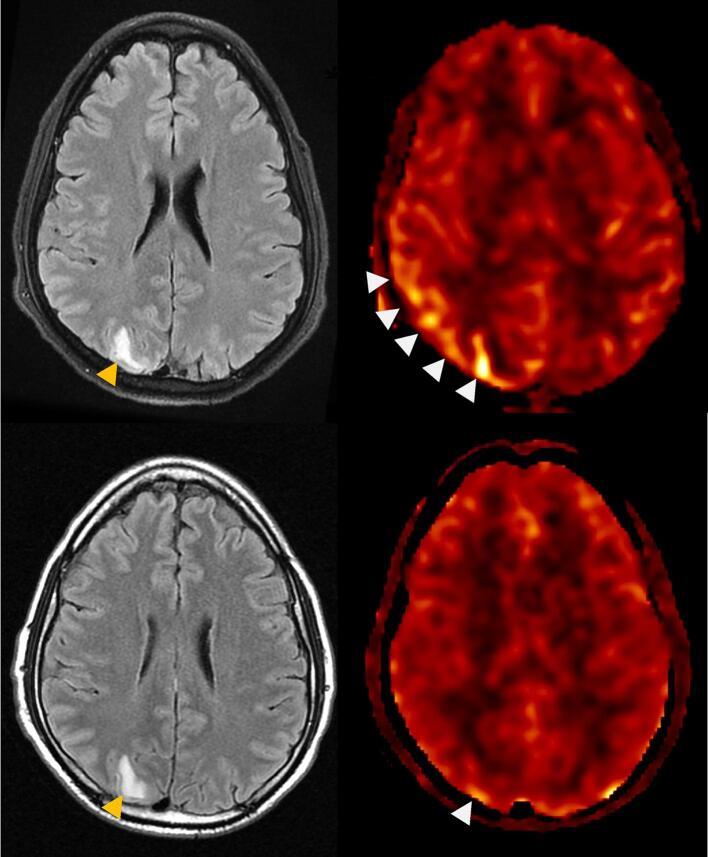
Materials and methods: After obtaining Institutional Review Board approval, MRI reports at our institution from 07/2015 to 09/2020 were retrospectively searched and reviewed for mention of "PRES" and "posterior reversible encephalopathy syndrome." Of the resulting 103 MRIs (performed on GE 1.5 Tesla or 3 Tesla scanners), 20 MRIs in 18 patients who met the inclusion criteria of clinical and imaging diagnosis of PRES and had diagnostic-quality pseudocontinuous ASL scans were included. Patients with a more likely alternative diagnosis, technically non-diagnostic ASL, or other intracranial abnormalities limiting assessment of underlying PRES features were excluded. Perfusion in FLAIR-affected brain regions was qualitatively assessed using ASL and characterized as hyperperfusion, normal, or hypoperfusion. Additional quantitative analysis was performed by measuring average gray matter CBF in abnormal versus normal brain regions.
Results: HTN was the most common PRES etiology (65%). ASL showed hyperperfusion in 13 cases and normal perfusion in 7 cases. A hypoperfusion pattern was not identified. Quantitative analysis of gray matter CBF among patients with visually apparent hyperperfusion showed statistically higher perfusion in affected versus normal appearing brain regions (median CBF 100.4 ml/100 g-min vs. 61.0 ml/ 100 g-min, p < 0.001).
Conclusion: Elevated ASL CBF was seen in the majority (65%) of patients with PRES, favoring the autoregulatory failure hypothesis as a predominant mechanism. Our data support ASL as a practical way to assess and noninvasively monitor cerebral perfusion in PRES that could potentially alter management strategies.
Keywords: ASL; Arterial spin labeling; CBF; Cerebral blood flow; PRES; Posterior reversible encephalopathy syndrome.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Figures




References
-
- Hinchey J., Chaves C., Appignani B., Breen J., Pao L., Wang A., Pessin M.S., Lamy C., Mas J.-L., Caplan L.R. A reversible posterior leukoencephalopathy syndrome. N. Engl. J. Med. 1996;334(8):494–500. - PubMed
Further reading
-
- Amukotuwa S.A., Yu C., Zaharchuk G. 3D Pseudocontinuous arterial spin labeling in routine clinical practice: a review of clinically significant artifacts. J. Magn. Reson. Imaging. 2016;43(1):11–27. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
