

Improved Outcomes of Thermal Ablation for Colorectal Liver Metastases: A 10-Year Analysis from the Prospective Amsterdam CORE Registry (AmCORE)
- PMID: 35585138
- PMCID: PMC9307533
- DOI: 10.1007/s00270-022-03152-9
Improved Outcomes of Thermal Ablation for Colorectal Liver Metastases: A 10-Year Analysis from the Prospective Amsterdam CORE Registry (AmCORE)
Abstract
Background: To analyze long-term oncological outcomes of open and percutaneous thermal ablation in the treatment of patients with colorectal liver metastases (CRLM).
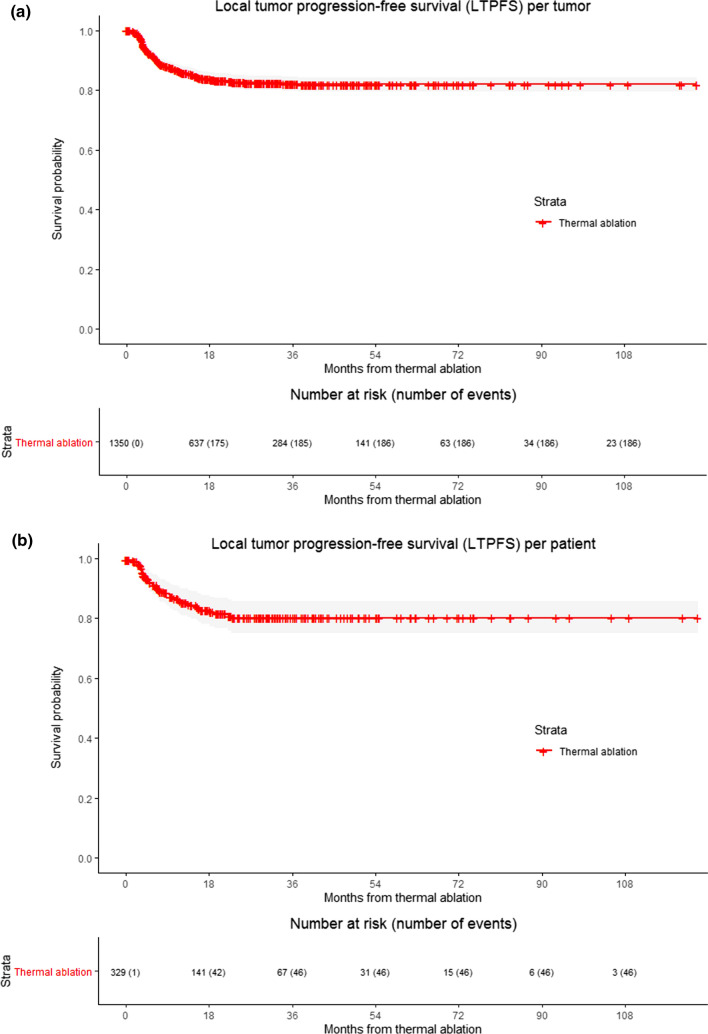
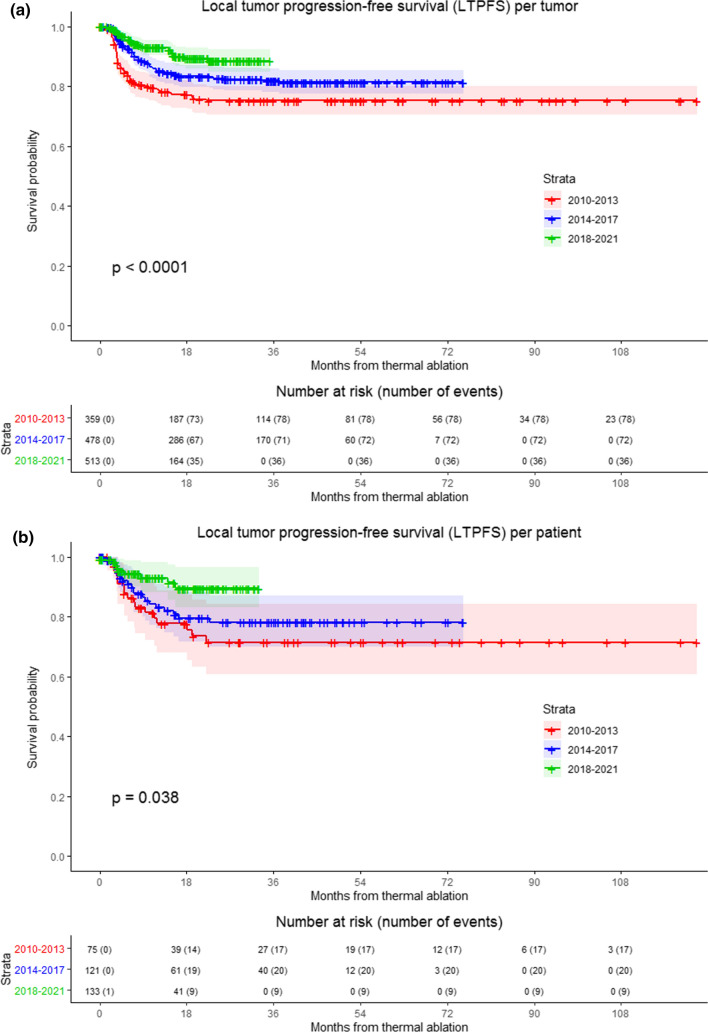
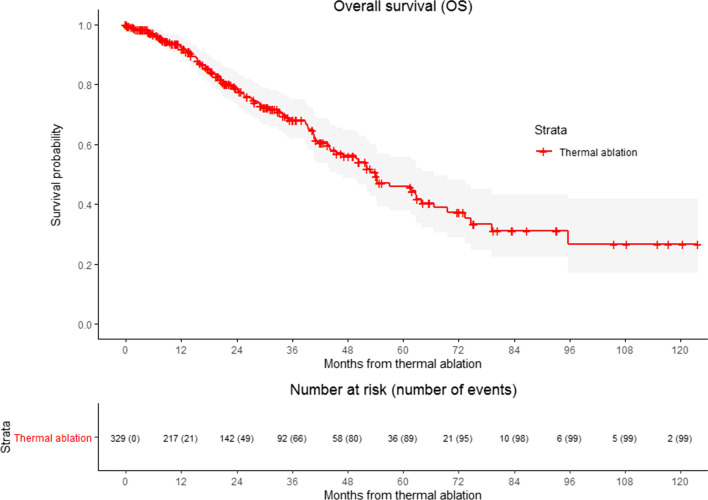
Methods: This assessment from a prospective, longitudinal tumor registry included 329 patients who underwent 541 procedures for 1350 CRLM from January 2010 to February 2021. Three cohorts were formed: 2010-2013 (129 procedures [53 percutaneous]), 2014-2017 (206 procedures [121 percutaneous]) and 2018-2021 (206 procedures [135 percutaneous]). Local tumor progression-free survival (LTPFS) and overall survival (OS) data were estimated using the Kaplan-Meier method. Potential confounding factors were analyzed with uni- and multivariable Cox regression analyses.
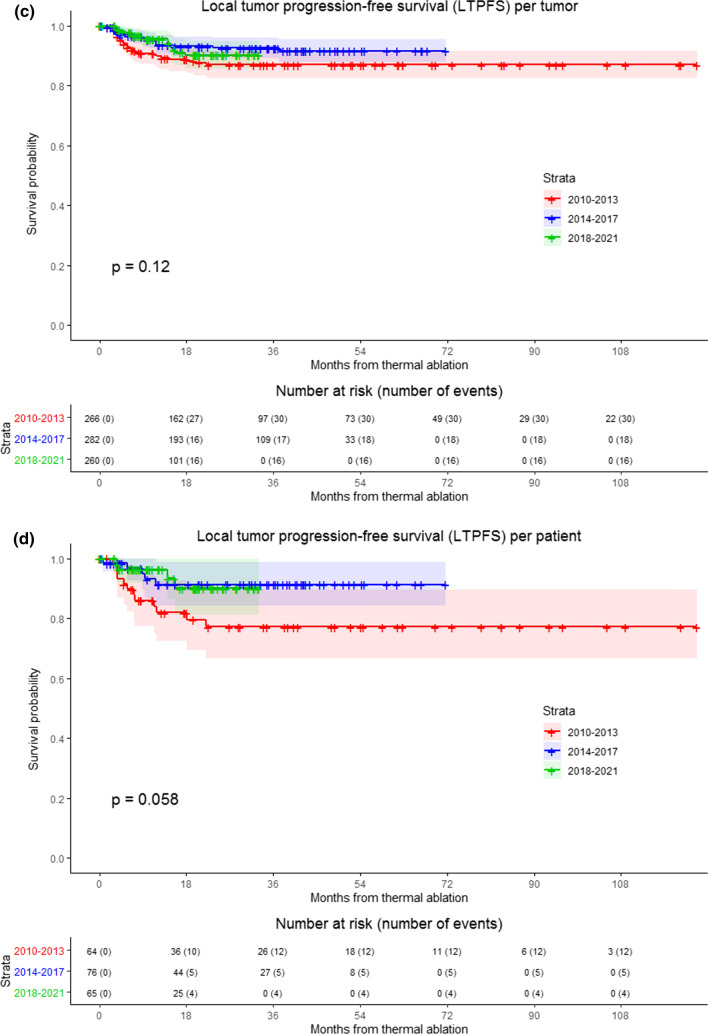
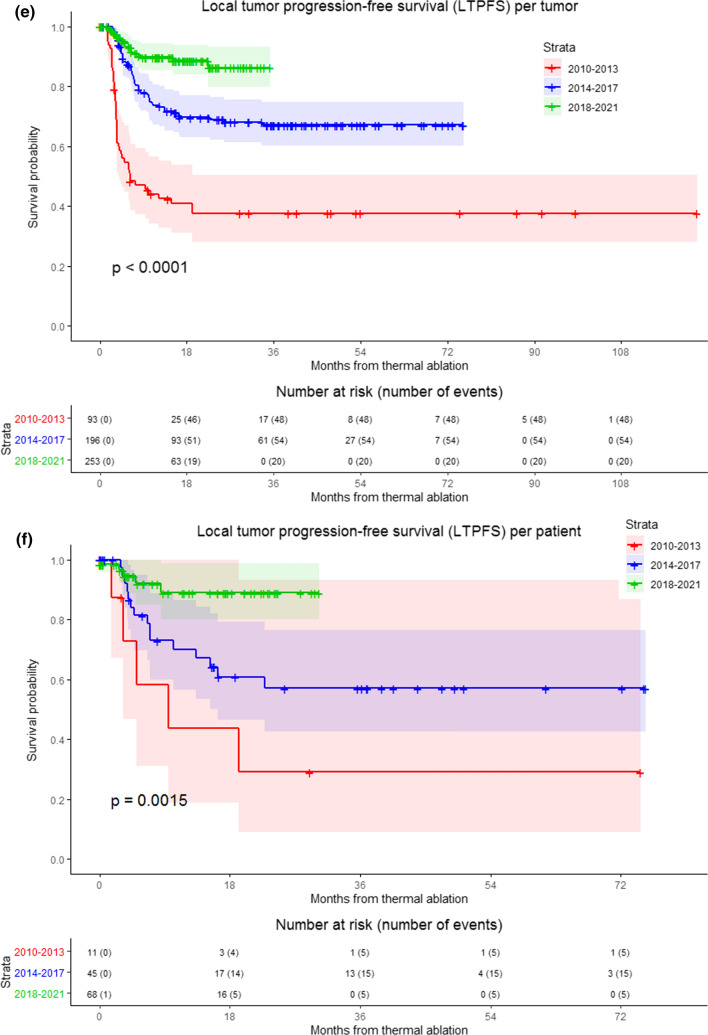
Results: LTPFS improved significantly over time for percutaneous ablations (2-year LTPFS 37.7% vs. 69.0% vs. 86.3%, respectively, P < .0001), while LTPFS for open ablations remained reasonably stable (2-year LTPFS 87.1% [2010-2013], vs. 92.7% [2014-2017] vs. 90.2% [2018-2021], P = .12). In the latter cohort (2018-2021), the open approach was no longer superior regarding LTPFS (P = .125). No differences between the three cohorts were found regarding OS (P = .088), length of hospital stay (open approach, P = .065; percutaneous approach, P = .054), and rate and severity of complications (P = .404). The rate and severity of complications favored the percutaneous approach in all three cohorts (P = .002).
Conclusion: Over the last 10 years efficacy of percutaneous ablations has improved remarkably for the treatment of CRLM. Oncological outcomes seem to have reached results following open ablation. Given its minimal invasive character and shorter length of hospital stay, whenever feasible, percutaneous procedures may be favored over an open approach.
Keywords: Colorectal liver metastases (CRLM); Local tumor progression-free survival (LTPFS); Long-term oncological outcomes; Microwave ablation (MWA); Radiofrequency ablation (RFA).
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Meijerink MR, Puijk RS, van Tilborg A, et al. Radiofrequency and microwave ablation compared to systemic chemotherapy and to partial hepatectomy in the treatment of colorectal liver metastases: a systematic review and meta-analysis. Cardiovasc Intervent Radiol. 2018;41:1189–1204. doi: 10.1007/s00270-018-1959-3. - DOI - PMC - PubMed
-
- Bala MM, Riemsma RP, Wolff R, et al. Microwave coagulation for liver metastases. Cochrane Database Syst Rev. 2013;1:010163. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
