

A rare case of synchronous multiple primary malignancies of breast cancer and diffuse large B-cell lymphoma that responded to multidisciplinary treatment: a case report
- PMID: 35585439
- PMCID: PMC9117581
- DOI: 10.1186/s40792-022-01456-z
A rare case of synchronous multiple primary malignancies of breast cancer and diffuse large B-cell lymphoma that responded to multidisciplinary treatment: a case report
Abstract
Background: Multiple primary malignancies of breast cancer and diffuse large B-cell lymphoma (DLBCL) are rare. Here, we report a case of advanced breast cancer and DLBCL managed with multidisciplinary therapy preceded by surgery with a successful outcome.
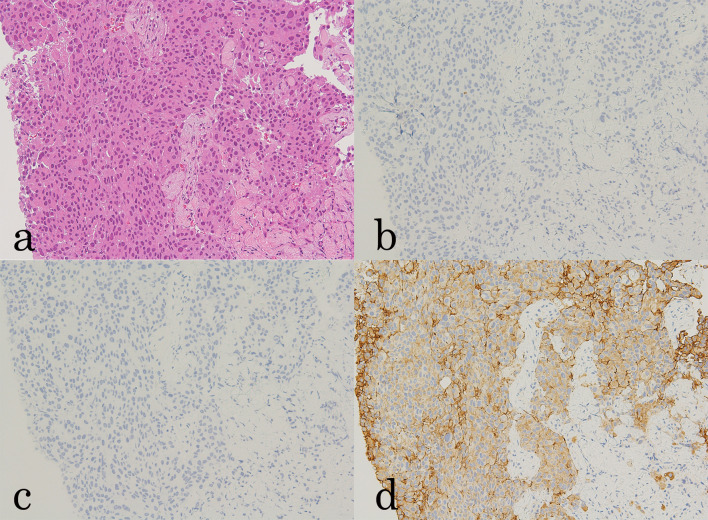
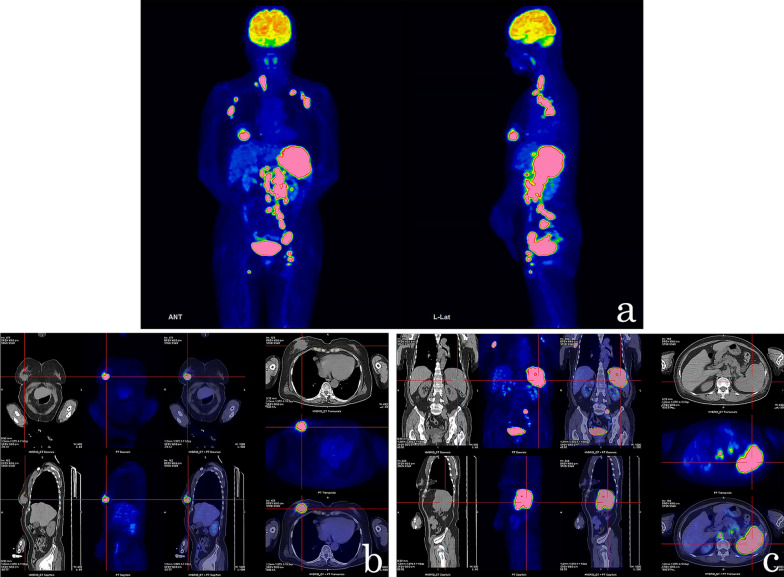
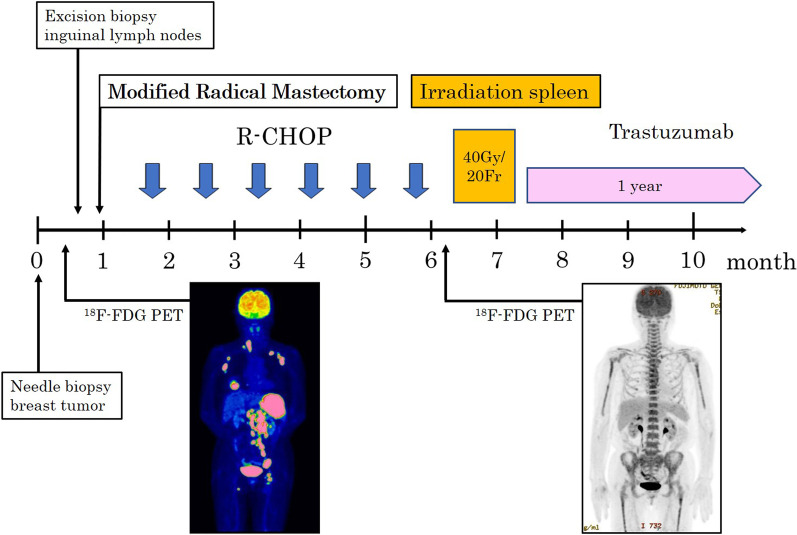
Case presentation: During a medical examination, a 71-year-old woman was diagnosed with a right breast mass, enlarged lymph nodes throughout the body, and a splenic tumor. The results of the clinical examination and imaging were suggestive of widely spread breast cancer with lymph node metastasis and malignant lymphoma with systemic metastasis. The histological evaluation of the biopsied breast tissue revealed human epidermal growth factor receptor 2 (HER2)-positive breast cancer, whereas the histological evaluation of the excised inguinal lymph node revealed DLBCL. 18F-FDG PET/computed tomography was performed, and it was determined that both breast cancer and DLBCL were in an advanced stage. Thus, mastectomy was performed, and the axillary lymph nodes showed mixed metastasis of breast cancer and DLBCL. Soon after, the R-CHOP therapy was initiated (375-mg/m2 rituximab, 2-mg/m2 vincristine, 50-mg/m2 doxorubicin, 750-mg/m2 cyclophosphamide, and 125-mg methylprednisolone). After irradiation of the spleen, trastuzumab was administered for 1 year.
Conclusions: We experienced a case of combined breast cancer and DLBCL, which was difficult to treat because both were in advanced stages. Thorough staging of the malignancy and discussion by a multidisciplinary team are necessary to determine the optimal treatment strategy.
Keywords: Breast cancer; DLBCL; Double cancer; Multiple primary malignancies; Synchronous.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Primary diffuse large B cell lymphoma of the lactating left breast. A case report and review of the literature.Ann Ital Chir. 2020 Dec 28;9:S2239253X20033101. Ann Ital Chir. 2020. PMID: 33427203 Review.
-
Synchronous Invasive Ductal Carcinoma of Breast and Diffuse Large B-cell Lymphoma: A Case Report.J Cancer Allied Spec. 2024 Aug 16;10(2):655. doi: 10.37029/jcas.v10i2.655. eCollection 2024. J Cancer Allied Spec. 2024. PMID: 39156944 Free PMC article.
-
[A Treatment Strategy against Double Presentation of Breast Cancer and Malignant Lymphoma].Gan To Kagaku Ryoho. 2018 Sep;45(9):1347-1351. Gan To Kagaku Ryoho. 2018. PMID: 30237379 Review. Japanese.
-
Synchronous occurrence of breast cancer and refractory diffuse large B-cell abdominal lymphoma: Management and review of the literature.Intractable Rare Dis Res. 2021 May;10(2):131-135. doi: 10.5582/irdr.2021.01017. Intractable Rare Dis Res. 2021. PMID: 33996360 Free PMC article.
-
Primary Splenic Diffuse Large B-cell Lymphoma: An Atypical Presentation.Cureus. 2023 Jun 22;15(6):e40793. doi: 10.7759/cureus.40793. eCollection 2023 Jun. Cureus. 2023. PMID: 37485157 Free PMC article.
Cited by
-
A Rare Case of Non-Hodgkin B-Cell Lymphoma Following Invasive Lobular Carcinoma of the Breast: A Case Report.Curr Oncol. 2025 Apr 10;32(4):218. doi: 10.3390/curroncol32040218. Curr Oncol. 2025. PMID: 40277774 Free PMC article.
-
Diagnosis and treatment of metachronous multiple primary carcinoma: A case report and review of literature.World J Clin Oncol. 2025 May 24;16(5):105444. doi: 10.5306/wjco.v16.i5.105444. World J Clin Oncol. 2025. PMID: 40503404 Free PMC article.
-
Two case reports of breast cancer combined with synchronous primary intrahepatic cholangiocarcinoma/mixed liver cancer.Medicine (Baltimore). 2024 Nov 29;103(48):e40653. doi: 10.1097/MD.0000000000040653. Medicine (Baltimore). 2024. PMID: 39612433 Free PMC article.
-
Breast Carcinoma Coexistent with Ipsilateral Axillary Non-Hodgkin Lymphoma: Cytological Diagnosis Aided with Cellblock Immunohistochemistry.Iran J Pathol. 2024 Spring;19(2):69-271. doi: 10.30699/IJP.2024.2014737.3203. Epub 2024 Feb 15. Iran J Pathol. 2024. PMID: 39118791 Free PMC article. No abstract available.
References
-
- Frei KA, Bonel HM, Forrer P, Alleman J, Steiner RA. Primary breast lymphoma, contralateral breast cancer, and bilateral Brenner tumors of the ovary. Obstet Gynecol. 2002;100:1079–1082. - PubMed
-
- Warren S, Gates O. Multiple malignant tumors. A survey of the literature and statistical study. Am J Cancer. 1932;16:1358–1414.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
