

A red flag for diagnosing brain death: decompressive craniectomy of the posterior fossa
- PMID: 35585474
- PMCID: PMC9279213
- DOI: 10.1007/s12630-022-02265-6
A red flag for diagnosing brain death: decompressive craniectomy of the posterior fossa
Abstract
Purpose: Brain death/death by neurologic criteria (BD/DNC) may be determined in many countries by a clinical examination that shows coma, brainstem areflexia, and apnea, provided the conditions causing reversible loss of brain function are excluded a priori. To date, accounts of recovery from BD/DNC in adults have been limited to noncompliance with guidelines.
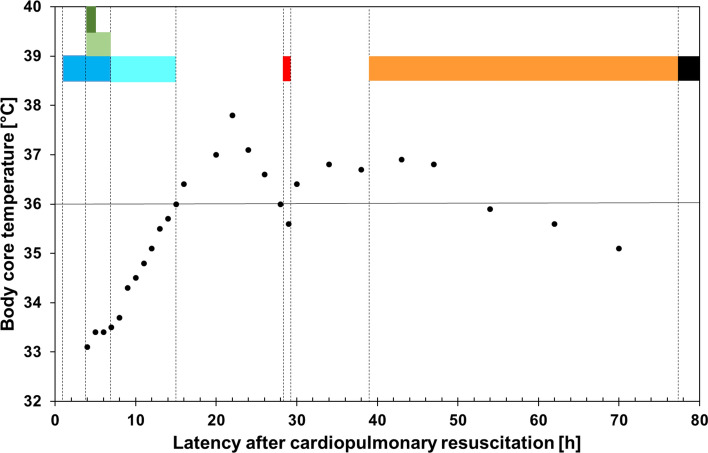
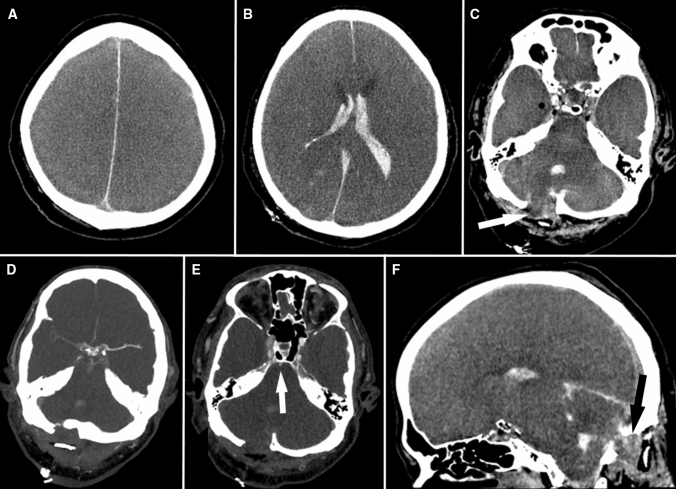
Clinical features: We report the case of a 72-yr-old man with a combined primary infratentorial (hemorrhagic) and secondary global (anoxic) brain lesion in whom decompressive craniectomy of the posterior fossa and six-hour therapeutic hypothermia (33-34°C) followed by 8-hour rewarming to ≥ 36°C were conducted. Thirteen hours later, clinical findings of brain function loss were documented in addition to guideline-compliant exclusion of reversible causes (arterial hypotension, intoxication, depressant drug effects, relevant metabolic or endocrine disequilibrium, chronic hypercapnia, neuromuscular disorders, and administration of a muscle relaxant). Since a primary infratentorial brain lesion was present, German guidelines required further ancillary testing. Doppler ultrasonography revealed some preserved cerebral circulation, and BD/DNC was not diagnosed. Approximately 24 hr after rewarming to ≥ 36°C, the patient exhibited respiratory efforts. He continued with assisted respiration until final asystole/apnea, without regaining additional brain function other than mild signs of hemispasticity. Follow-up computed tomography showed partial herniation of the cerebellum through the craniectomy gap of the posterior fossa, alleviating caudal brain stem compression.
Conclusions: Therapeutic decompressive craniectomy of the posterior fossa may allow for delayed reversal of apnea. In these patients, proof of cerebral circulatory arrest should be mandatory for diagnosing BD/DNC.
RéSUMé: OBJECTIF: Dans de nombreux pays, la mort cérébrale / décès déterminé par des critères neurologiques (MC / DDN) peut être déterminée par un examen clinique qui montre le coma, l’aréflexie du tronc cérébral et l’apnée, sous réserve que les conditions causant une perte réversible de la fonction cérébrale soient exclues a priori. À ce jour, les comptes rendus décrivant un rétablissement après une MC / DDN chez les adultes ont été limités en raison d’un non-respect des lignes directrices. CARACTéRISTIQUES CLINIQUES: Nous rapportons le cas d’un homme de 72 ans atteint d’une lésion cérébrale sous-tentorielle primaire (hémorragique) et secondaire globale (anoxique) chez qui une craniectomie décompressive de la fosse postérieure et une hypothermie thérapeutique de six heures (33-34 °C), suivie d’un réchauffement de 8 heures à ≥ 36 °C, ont été réalisés. Treize heures plus tard, les résultats cliniques de la perte de la fonction cérébrale ont été documentés, en plus de l’exclusion conforme aux lignes directrices des causes réversibles (hypotension artérielle, intoxication, effets des médicaments dépresseurs, déséquilibre métabolique ou endocrinien pertinent, hypercapnie chronique, troubles neuromusculaires et administration d’un relaxant musculaire). Étant donné qu’une lésion cérébrale sous-tentorielle primaire était présente, les directives allemandes exigeaient la réalisation d’autres tests auxiliaires. L’échographie Doppler a révélé la préservation d’une certaine circulation cérébrale, et la MC / DDN n’a pas été diagnostiquée. Environ 24 heures après le réchauffement du patient à ≥ 36 °C, le patient a manifesté des efforts respiratoires. Il a continué à respirer avec assistance jusqu’à l’asystole / l’apnée finale, sans retrouver de fonction cérébrale supplémentaire autre que de légers signes d’hémispasticité. La tomodensitométrie de suivi a montré une hernie partielle du cervelet à travers l’espace de craniectomie de la fosse postérieure, soulageant la compression caudale du tronc cérébral. CONCLUSION: La craniectomie décompressive thérapeutique de la fosse postérieure peut permettre une inversion retardée de l’apnée. Chez ces patients, la preuve d’un arrêt circulatoire cérébral devrait être obligatoire pour diagnostiquer une MC / DDN.
Keywords: Doppler ultrasonography; brain death; cerebellar hematoma; cessation of brain function; computed tomography angiography; electroencephalography.
© 2022. The Author(s).
Figures
Comment in
-
Decompressive craniectomy as a potentially reversible condition in brain death-brain stunning or skin and pericranium stretching?Can J Anaesth. 2022 Jul;69(7):811-814. doi: 10.1007/s12630-022-02264-7. Epub 2022 May 10. Can J Anaesth. 2022. PMID: 35534771 English. No abstract available.
-
Withholding therapeutic interventions in brain(stem) death: is it a self-fulfilling prophecy?Can J Anaesth. 2022 Nov;69(11):1435-1436. doi: 10.1007/s12630-022-02324-y. Epub 2022 Sep 12. Can J Anaesth. 2022. PMID: 36097130 No abstract available.
-
In reply: Withholding therapeutic interventions in brain(stem) death: is it a self-fulfilling prophecy?Can J Anaesth. 2022 Nov;69(11):1437-1438. doi: 10.1007/s12630-022-02325-x. Epub 2022 Sep 12. Can J Anaesth. 2022. PMID: 36097132 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
