

Do functional status and Medicare claims data improve the predictive accuracy of an electronic health record mortality index? Findings from a national Veterans Affairs cohort
- PMID: 35585537
- PMCID: PMC9118715
- DOI: 10.1186/s12877-022-03126-z
Do functional status and Medicare claims data improve the predictive accuracy of an electronic health record mortality index? Findings from a national Veterans Affairs cohort
Abstract
Background: Electronic health record (EHR) prediction models may be easier to use in busy clinical settings since EHR data can be auto-populated into models. This study assessed whether adding functional status and/or Medicare claims data (which are often not available in EHRs) improves the accuracy of a previously developed Veterans Affairs (VA) EHR-based mortality index.
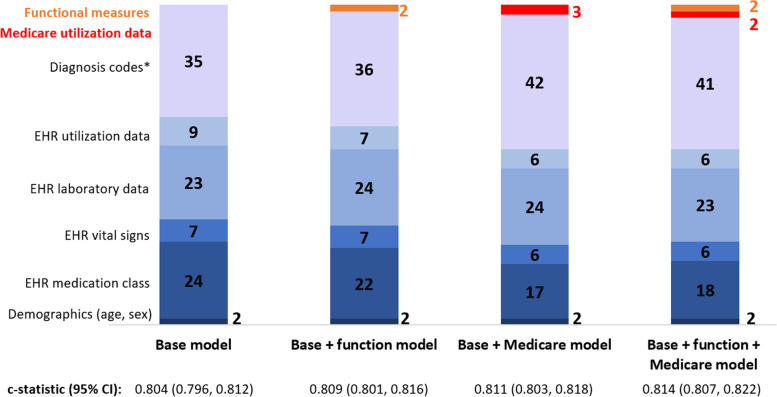
Methods: This was a retrospective cohort study of veterans aged 75 years and older enrolled in VA primary care clinics followed from January 2014 to April 2020 (n = 62,014). We randomly split participants into development (n = 49,612) and validation (n = 12,402) cohorts. The primary outcome was all-cause mortality. We performed logistic regression with backward stepwise selection to develop a 100-predictor base model using 854 EHR candidate variables, including demographics, laboratory values, medications, healthcare utilization, diagnosis codes, and vitals. We incorporated functional measures in a base + function model by adding activities of daily living (range 0-5) and instrumental activities of daily living (range 0-7) scores. Medicare data, including healthcare utilization (e.g., emergency department visits, hospitalizations) and diagnosis codes, were incorporated in a base + Medicare model. A base + function + Medicare model included all data elements. We assessed model performance with the c-statistic, reclassification metrics, fraction of new information provided, and calibration plots.
Results: In the overall cohort, mean age was 82.6 years and 98.6% were male. At the end of follow-up, 30,263 participants (48.8%) had died. The base model c-statistic was 0.809 (95% CI 0.805-0.812) in the development cohort and 0.804 (95% CI 0.796-0.812) in the validation cohort. Validation cohort c-statistics for the base + function, base + Medicare, and base + function + Medicare models were 0.809 (95% CI 0.801-0.816), 0.811 (95% CI 0.803-0.818), and 0.814 (95% CI 0.807-0.822), respectively. Adding functional status and Medicare data resulted in similarly small improvements among other model performance measures. All models showed excellent calibration.
Conclusions: Incorporation of functional status and Medicare data into a VA EHR-based mortality index led to small but likely clinically insignificant improvements in model performance.
Keywords: Functional status; Medicare data; Mortality prediction model; Physical function.
© 2022. The Author(s).
Conflict of interest statement
The authors report no competing interests. The views expressed in this article are those of the authors and do not necessarily represent the views of the Veterans Affairs or the United States government.
Figures
References
-
- ePrognosis. https://eprognosis.ucsf.edu/. Accessed 5 Apr 2022.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
