

Medical nutrition therapy and clinical outcomes in critically ill adults: a European multinational, prospective observational cohort study (EuroPN)
- PMID: 35585554
- PMCID: PMC9115983
- DOI: 10.1186/s13054-022-03997-z
Medical nutrition therapy and clinical outcomes in critically ill adults: a European multinational, prospective observational cohort study (EuroPN)
Abstract
Background: Medical nutrition therapy may be associated with clinical outcomes in critically ill patients with prolonged intensive care unit (ICU) stay. We wanted to assess nutrition practices in European intensive care units (ICU) and their importance for clinical outcomes.
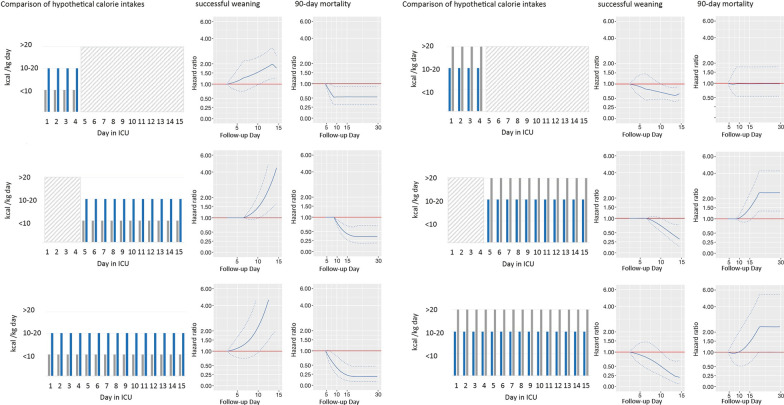
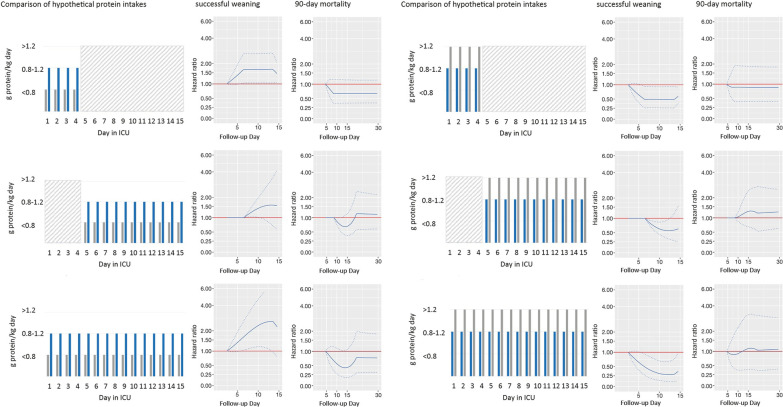
Methods: Prospective multinational cohort study in patients staying in ICU ≥ 5 days with outcome recorded until day 90. Macronutrient intake from enteral and parenteral nutrition and non-nutritional sources during the first 15 days after ICU admission was compared with targets recommended by ESPEN guidelines. We modeled associations between three categories of daily calorie and protein intake (low: < 10 kcal/kg, < 0.8 g/kg; moderate: 10-20 kcal/kg, 0.8-1.2 g/kg, high: > 20 kcal/kg; > 1.2 g/kg) and the time-varying hazard rates of 90-day mortality or successful weaning from invasive mechanical ventilation (IMV).
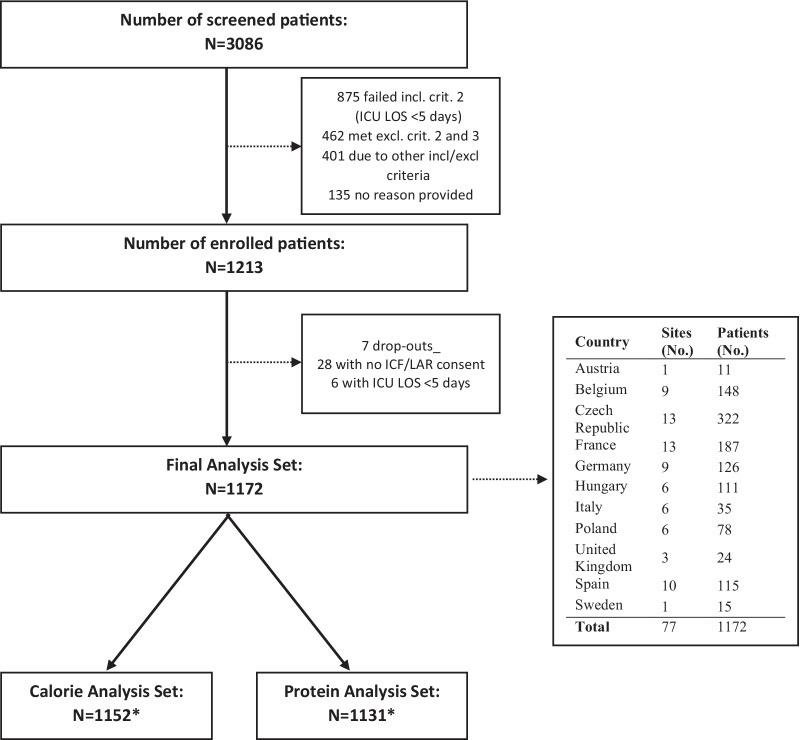
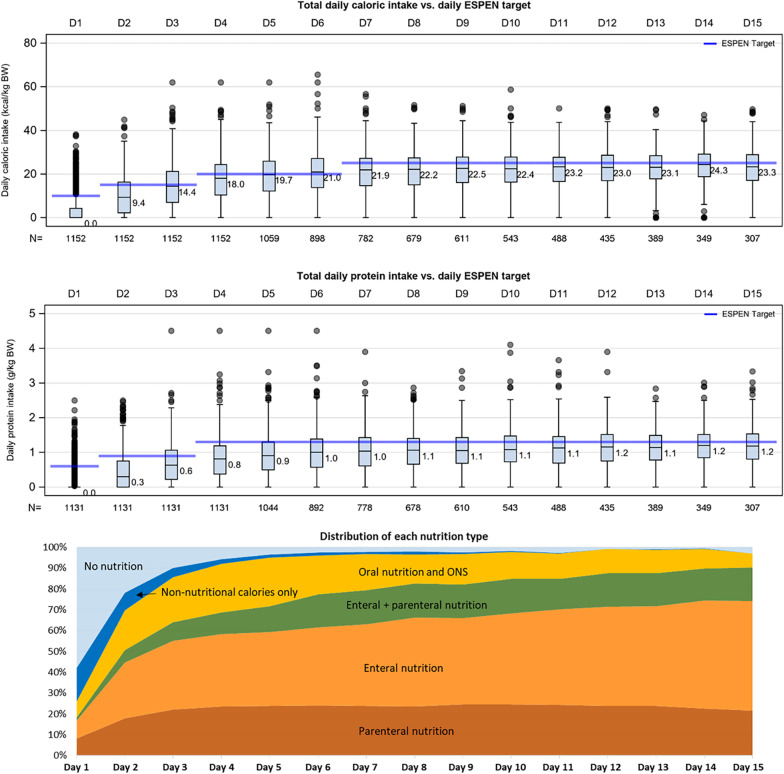
Results: A total of 1172 patients with median [Q1;Q3] APACHE II score of 18.5 [13.0;26.0] were included, and 24% died within 90 days. Median length of ICU stay was 10.0 [7.0;16.0] days, and 74% of patients could be weaned from invasive mechanical ventilation. Patients reached on average 83% [59;107] and 65% [41;91] of ESPEN calorie and protein recommended targets, respectively. Whereas specific reasons for ICU admission (especially respiratory diseases requiring IMV) were associated with higher intakes (estimate 2.43 [95% CI: 1.60;3.25] for calorie intake, 0.14 [0.09;0.20] for protein intake), a lack of nutrition on the preceding day was associated with lower calorie and protein intakes (- 2.74 [- 3.28; - 2.21] and - 0.12 [- 0.15; - 0.09], respectively). Compared to a lower intake, a daily moderate intake was associated with higher probability of successful weaning (for calories: maximum HR 4.59 [95% CI: 1.5;14.09] on day 12; for protein: maximum HR 2.60 [1.09;6.23] on day 12), and with a lower hazard of death (for calories only: minimum HR 0.15, [0.05;0.39] on day 19). There was no evidence that a high calorie or protein intake was associated with further outcome improvements.
Conclusions: Calorie intake was mainly provided according to the targets recommended by the active ESPEN guideline, but protein intake was lower. In patients staying in ICU ≥ 5 days, early moderate daily calorie and protein intakes were associated with improved clinical outcomes. Trial registration NCT04143503 , registered on October 25, 2019.
Keywords: Calorie; Critical illness; Mechanical ventilation; Nutrition; Protein; Survival; Weaning.
© 2022. The Author(s).
Conflict of interest statement
M. Hiesmayr has received lecture fees and travel support from Fresenius Kabi, Nestlé, Baxter, SSPC, consulting fees from Fresenius Kabi, and unrestricted research grants from Baxter and Fresenius Kabi to Medical University Vienna. M. Matejovic has received lecture fees from Fresenius Kabi, Baxter, Nutricia and consulting fees and travel support from Fresenius Kabi. C. Vaquerizo has received lecture fees and travel support from Fresenius Kabi, Nestlé Healthcare Nutrition, Abbott Nutrition and Vegenat Nutrisens and consulting fees from Fresenius Kabi and Vegenat Nutrisens. G. Elke has received lecture fees and travel support from Fresenius Kabi, Baxter and consulting fees and travel support from Cardinal Health, Fresenius Kabi, and Nutricia. K. Dams has received lecture fees from Fresenius Kabi, Baxter, Nestlé and consulting fees and travel support from Fresenius Kabi. R. Tetamo has received lecture fees and travel support from Fresenius Kabi. W. Hartl has received travel support from Fresenius Kabi. H. Kuechenhoff has received travel support and consulting fees from Fresenius Kabi. O. Rooyackers has received lecture and consulting fees from Fresenius-Kabi, Nutricia, Nestle, and Baxter. The rest of the authors have no conflicts of interest to declare in relation to this study.
Figures
Similar articles
-
Route of nutrition and risk of blood stream infections in critically ill patients; a comparative study.Clin Nutr ESPEN. 2016 Apr;12:e14-e19. doi: 10.1016/j.clnesp.2016.01.002. Epub 2016 Mar 2. Clin Nutr ESPEN. 2016. PMID: 28531664
-
Calorie intake and short-term survival of critically ill patients.Clin Nutr. 2019 Apr;38(2):660-667. doi: 10.1016/j.clnu.2018.04.005. Epub 2018 Apr 18. Clin Nutr. 2019. PMID: 29709380
-
Nutritional practices and their relationship to clinical outcomes in critically ill children--an international multicenter cohort study*.Crit Care Med. 2012 Jul;40(7):2204-11. doi: 10.1097/CCM.0b013e31824e18a8. Crit Care Med. 2012. PMID: 22564954 Free PMC article.
-
Reconciling divergent results of the latest parenteral nutrition studies in the ICU.Curr Opin Clin Nutr Metab Care. 2013 Mar;16(2):187-93. doi: 10.1097/MCO.0b013e32835c34be. Curr Opin Clin Nutr Metab Care. 2013. PMID: 23385424 Review.
-
High vs low protein intake in chronic critical illness: A systematic review and meta-analysis.Clin Nutr ESPEN. 2025 Feb;65:249-255. doi: 10.1016/j.clnesp.2024.12.003. Epub 2024 Dec 9. Clin Nutr ESPEN. 2025. PMID: 39662588
Cited by
-
The effects of higher versus lower protein delivery in critically ill patients: an updated systematic review and meta-analysis of randomized controlled trials with trial sequential analysis.Crit Care. 2024 Jan 6;28(1):15. doi: 10.1186/s13054-023-04783-1. Crit Care. 2024. PMID: 38184658 Free PMC article.
-
Efficacy of permissive underfeeding for critically ill patients: an updated systematic review and trial sequential meta-analysis.J Intensive Care. 2024 Jan 23;12(1):4. doi: 10.1186/s40560-024-00717-3. J Intensive Care. 2024. PMID: 38254228 Free PMC article.
-
Comment: Early nutrition prescription in critically ill patients-learnings from the FRANS study.Crit Care. 2023 Feb 20;27(1):64. doi: 10.1186/s13054-023-04346-4. Crit Care. 2023. PMID: 36803191 Free PMC article. No abstract available.
-
Nutrition intake in critically ill patients with coronavirus disease (COVID-19): A nationwide, multicentre, observational study in Argentina.Endocrinol Diabetes Nutr (Engl Ed). 2023 Apr;70(4):245-254. doi: 10.1016/j.endien.2023.03.016. Endocrinol Diabetes Nutr (Engl Ed). 2023. PMID: 37116970 Free PMC article.
-
Association of early dietary fiber intake and mortality in septic patients with mechanical ventilation based on MIMIC IV 2.1 database: a cohort study.Nutr J. 2024 Jan 3;23(1):1. doi: 10.1186/s12937-023-00894-1. Nutr J. 2024. PMID: 38167155 Free PMC article.
References
-
- Lee Z-Y, Yap CSL, Hasan MS, Engkasan JP, Barakatun-Nisak MY, Day AG, et al. The effect of higher versus lower protein delivery in critically ill patients: a systematic review and meta-analysis of randomized controlled trials. Crit Care. 2021;25(1):1–15. doi: 10.1186/s13054-021-03693-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
