

The impact of COVID-19 vaccination in prisons in England and Wales: a metapopulation model
- PMID: 35585575
- PMCID: PMC9115545
- DOI: 10.1186/s12889-022-13219-4
The impact of COVID-19 vaccination in prisons in England and Wales: a metapopulation model
Abstract
Background: High incidence of cases and deaths due to coronavirus disease 2019 (COVID-19) have been reported in prisons worldwide. This study aimed to evaluate the impact of different COVID-19 vaccination strategies in epidemiologically semi-enclosed settings such as prisons, where staff interact regularly with those incarcerated and the wider community.
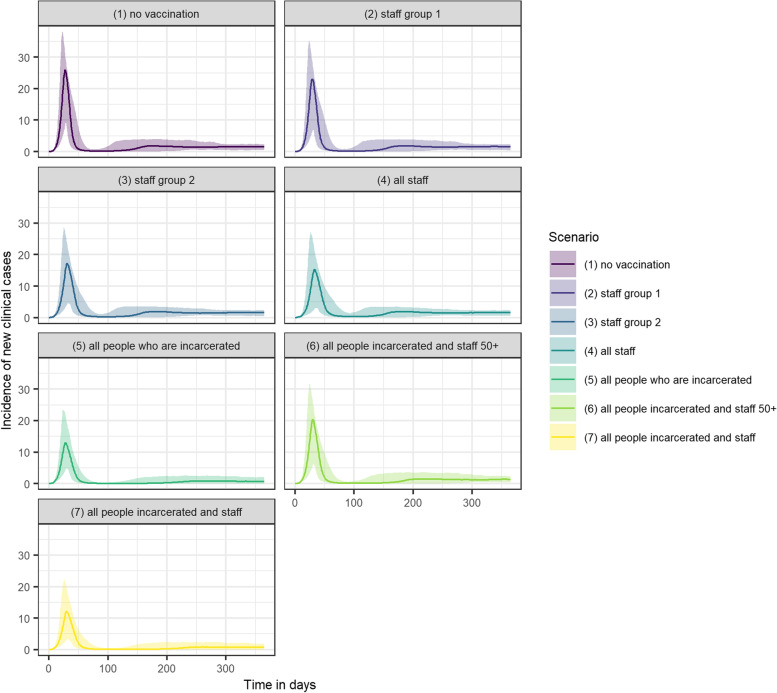
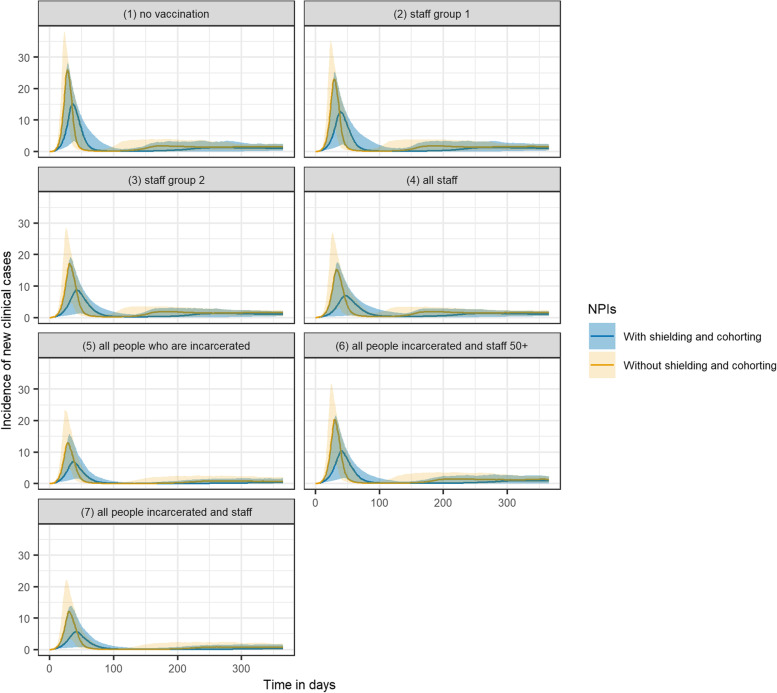
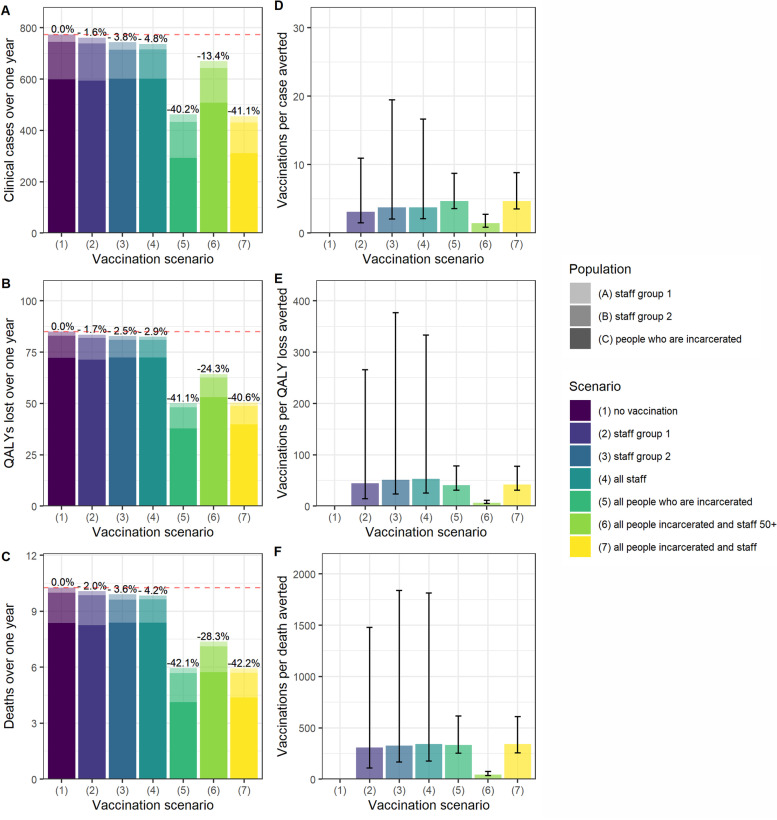
Methods: We used a metapopulation transmission-dynamic model of a local prison in England and Wales. Two-dose vaccination strategies included no vaccination, vaccination of all individuals who are incarcerated and/or staff, and an age-based approach. Outcomes were quantified in terms of COVID-19-related symptomatic cases, losses in quality-adjusted life-years (QALYs), and deaths.
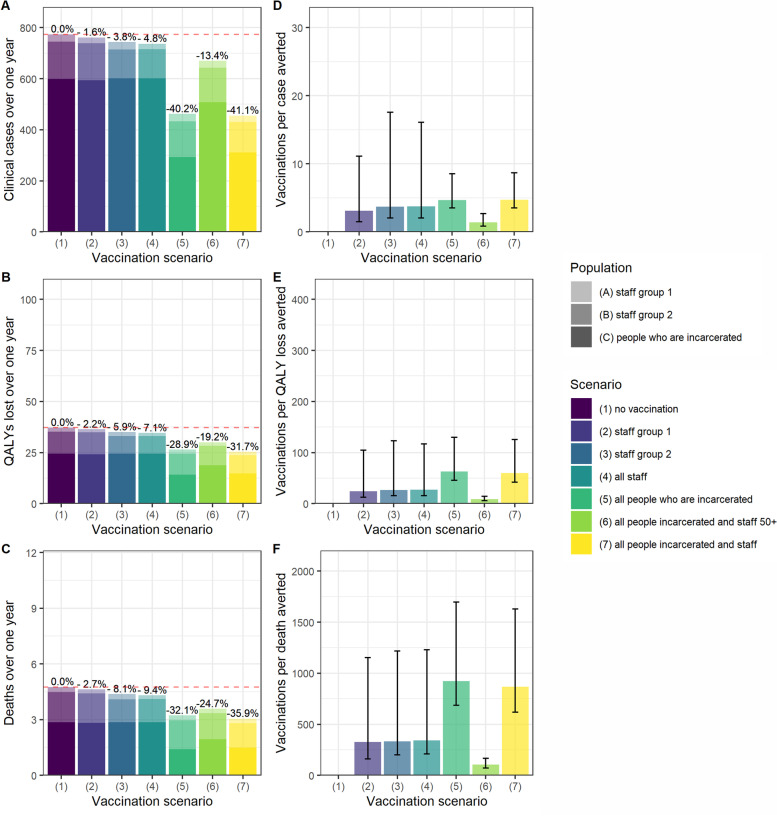
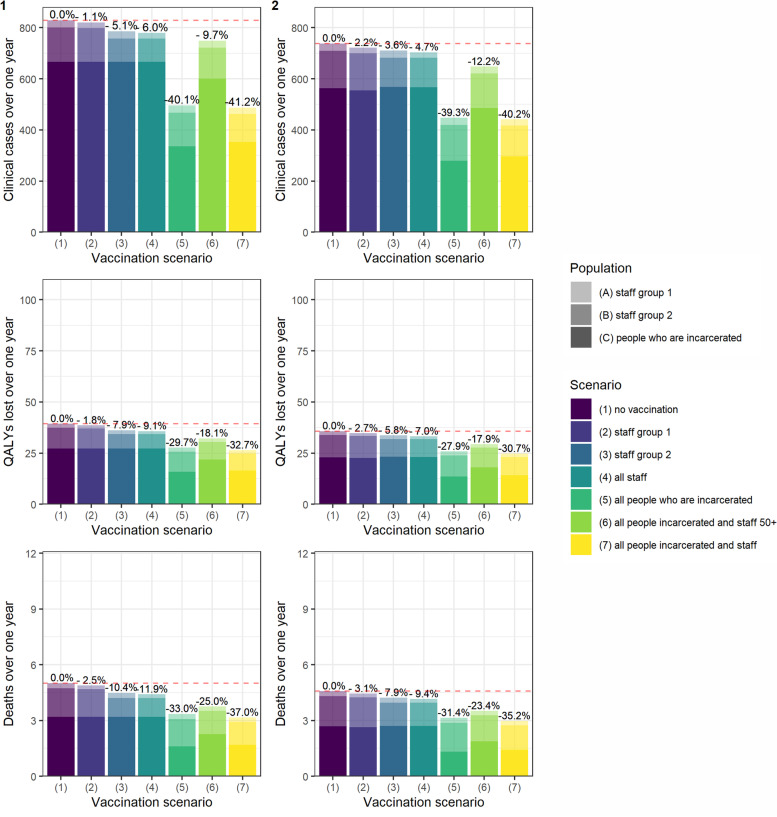
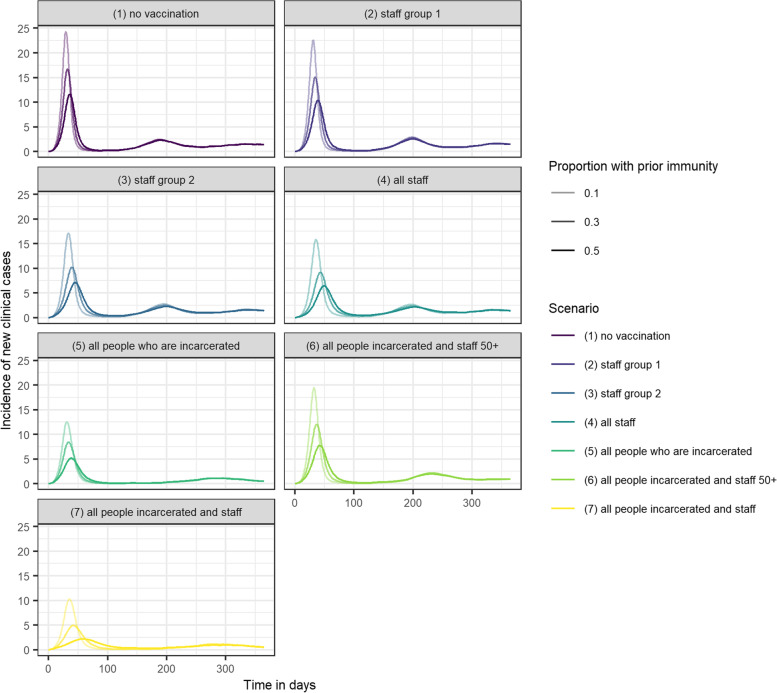
Results: Compared to no vaccination, vaccinating all people living and working in prison reduced cases, QALY loss and deaths over a one-year period by 41%, 32% and 36% respectively. However, if vaccine introduction was delayed until the start of an outbreak, the impact was negligible. Vaccinating individuals who are incarcerated and staff over 50 years old averted one death for every 104 vaccination courses administered. All-staff-only strategies reduced cases by up to 5%. Increasing coverage from 30 to 90% among those who are incarcerated reduced cases by around 30 percentage points.
Conclusions: The impact of vaccination in prison settings was highly dependent on early and rapid vaccine delivery. If administered to both those living and working in prison prior to an outbreak occurring, vaccines could substantially reduce COVID-19-related morbidity and mortality in prison settings.
Keywords: COVID-19; Mathematical model; Prisons; Public health; Vaccination.
© 2022. The Author(s).
Conflict of interest statement
O.O’M. is employed by Her Majesty's Prison and Probation Service. All other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
