

Comparison of cardiovascular outcomes between SGLT2 inhibitors in diabetes mellitus
- PMID: 35585590
- PMCID: PMC9115977
- DOI: 10.1186/s12933-022-01508-6
Comparison of cardiovascular outcomes between SGLT2 inhibitors in diabetes mellitus
Abstract
Background: There have been scarce data comparing cardiovascular outcomes between individual sodium-glucose cotransporter-2 (SGLT2) inhibitors. We aimed to compare the subsequent cardiovascular risk between individual SGLT2 inhibitors.
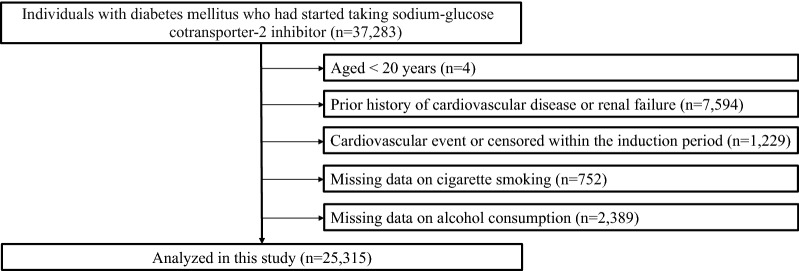
Methods: We analyzed 25,315 patients with diabetes mellitus (DM) newly taking SGLT2 inhibitors (empagliflozin: 5302, dapagliflozin: 4681, canagliflozin: 4411, other SGLT2 inhibitors: 10,921). We compared the risks of developing heart failure (HF), myocardial infarction (MI), angina pectoris (AP), stroke, and atrial fibrillation (AF) between individual SGLT2 inhibitors.
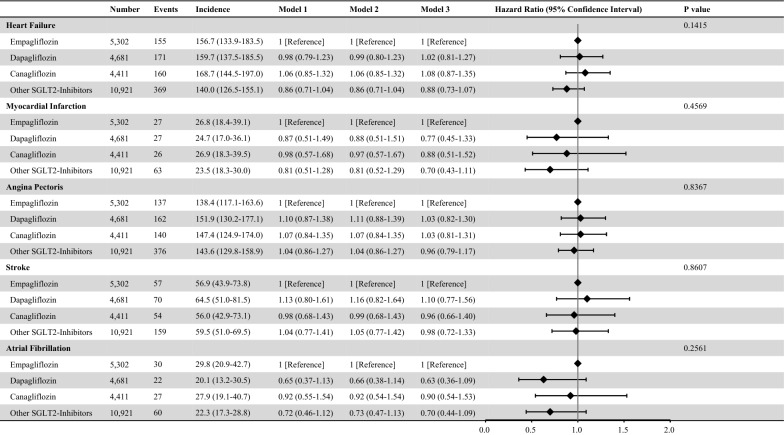
Results: Median age was 52 years, and 82.5% were men. The median fasting plasma glucose and HbA1c levels were 149 (Q1-Q3:127-182) mg/dL and 7.5 (Q1-Q3:6.9-8.6) %. During a mean follow-up of 814 ± 591 days, 855 HF, 143 MI, 815 AP, 340 stroke, and 139 AF events were recorded. Compared with empagliflozin, the risk of developing HF, MI, AP, stroke, and AF was not significantly different in dapagliflozin, canagliflozin, and other SGLT inhibitors. For developing HF, compared with empagliflozin, hazard ratios of dapagliflozin, canagliflozin, and other SGLT2 inhibitors were 1.02 (95% confidence interval [CI] 0.81-1.27), 1.08 (95% CI 0.87-1.35), and 0.88 (95% CI 0.73-1.07), respectively. Wald tests showed that there was no significant difference in the risk of developing HF, MI, AP, stroke, and AF among individual SGLT2 inhibitors. We confirmed the robustness of these results through a multitude of sensitivity analyses.
Conclusion: The risks for subsequent development of HF, MI, AP, stroke, and AF were comparable between individual SGLT2 inhibitors. This is the first study comparing the wide-range cardiovascular outcomes of patients with DM treated with individual SGLT2 inhibitors using large-scale real-world data.
Keywords: Cardiovascular disease; Diabetes mellitus; SGLT2 inhibitor.
© 2022. The Author(s).
Conflict of interest statement
Research funding and scholarship funds (Hidehiro Kaneko and Katsuhito Fujiu) from Medtronic Japan; Biotronik Japan; SIMPLEX QUANTUM; Boston Scientific Japan; and Fukuda Denshi, Central Tokyo. Akira Okada is a member of the Department of Prevention of Diabetes and Lifestyle-related Diseases, which is a cooperative program between The University of Tokyo and Asahi Mutual Life Insurance Company. The remaining authors have nothing to disclose.
Figures
References
-
- Buse JB, Wexler DJ, Tsapas A, et al. Update to management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia. 2019;63(2020):221–228. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
