

Atrial fibrillation in cancer patients who develop stroke
- PMID: 35585638
- PMCID: PMC9116009
- DOI: 10.1186/s40959-022-00137-y
Atrial fibrillation in cancer patients who develop stroke
Abstract
Background: Acute ischemic stroke (Stroke) and transient ischemic attacks (TIA) are known complications in cancer patients and those with atrial fibrillation (AF). The role AF plays in Stroke/TIA in the setting of cancer is unclear. The purpose of this study was to assess the relationship between AF and Stroke/TIA in cancer patients.
Methods: We conducted a case-control study comparing all patients who developed Stroke/TIA from 2014 to 2019 following a cancer diagnosis at King Hussein Cancer Center (KHCC), matched to Stroke/TIA-free controls based on age, gender, and cancer site.
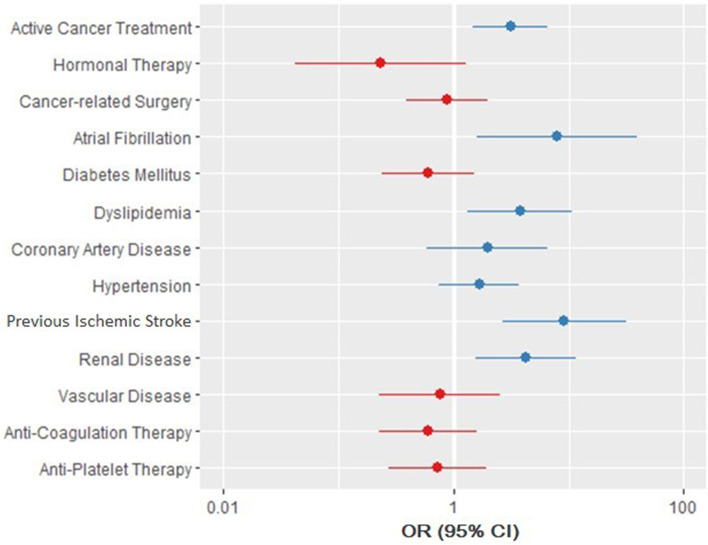
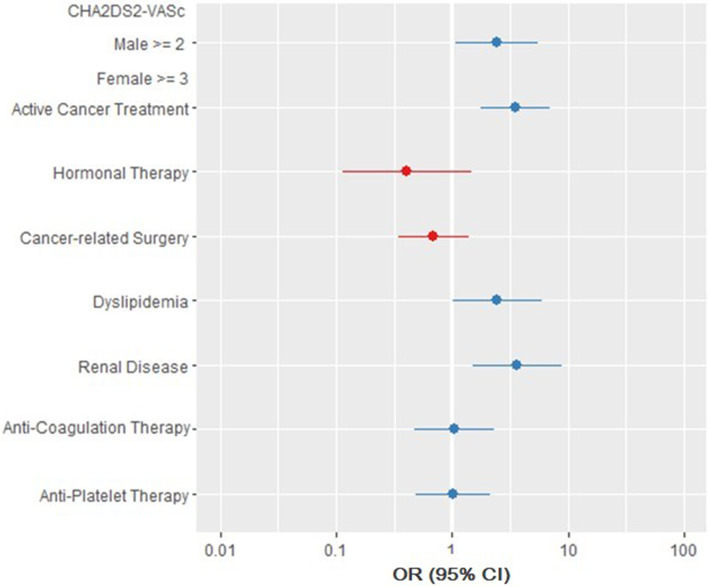
Results: Two hundred seventy-two patients were included (136 per group). The mean age was 63.95 ± 13.06 and 57% were females. The Stroke/TIA group had more AF at the time of event (14% vs. 4%, OR: 4.25, 95%-CI: 1.39 - 17.36) and had a larger proportion of death on study conclusion (OR: 9.4, 95%-CI: 3.74 - 23.64). On conditional logistic regression, patients in the Stroke/TIA group had higher odds of: AF (OR: 7.93, 95%-CI: 1.6 - 39.18), ischemic stroke before cancer diagnosis (OR: 9.18, 95%-CI: 2.66 - 31.74), being on active cancer treatment (OR: 3.11, 95%-CI: 1.46 - 6.62), dyslipidemia (OR: 3.78, 95%-CI: 1.32 - 10.82), and renal disease (OR: 4.25, 95%-CI: 1.55 - 11.63). On another conditional logistic regression model built to assess the role of the CHA2DS2-VASc score, a score of >=2 in males and >=3 in females significantly increased the risk of developing Stroke/TIA in cancer patients (OR: 2.45, 95%-CI: 1.08 - 5.58).
Conclusion: AF, previous ischemic stroke, active cancer treatment, dyslipidemia, and renal disease are independent risk factors for Stroke/TIA and a higher CHA2DS2-VASc score significantly increases the risk in cancer patients regardless of AF.
Keywords: Atrial fibrillation; Cancer; Ischemic stroke; Transient ischemic attack.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources