

Comparison of Contrast-Enhanced Spectral Mammography and Contrast-Enhanced MRI in Screening Multifocal and Multicentric Lesions in Breast Cancer Patients
- PMID: 35585943
- PMCID: PMC9007694
- DOI: 10.1155/2022/4224701
Comparison of Contrast-Enhanced Spectral Mammography and Contrast-Enhanced MRI in Screening Multifocal and Multicentric Lesions in Breast Cancer Patients
Abstract
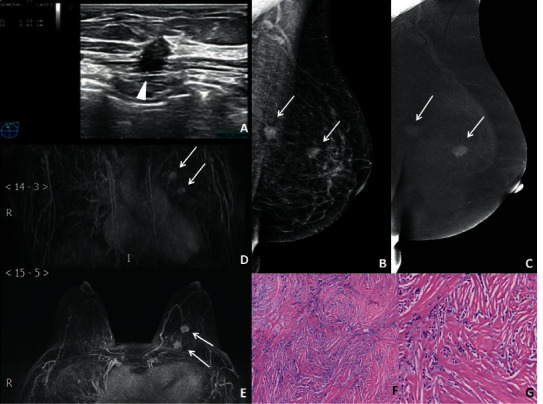
Objectives: We aimed to determine the difference between contrast-enhanced spectral mammography (CESM) and contrast-enhanced magnetic resonance imaging (CE-MRI) in detecting multifocal and multicentric breast cancer (MMBC).
Methods: : This study was conducted among breast cancer patients between July 1, 2017, and May 30, 2021. The sensitivity, specificity, and accuracy of CESM and CE-MRI in the diagnosis of MMBC were evaluated with pathological results as the gold standard.
Results: A total of 188 lesions were detected in 54 patients with MMBC, including 177 breast cancer and 11 benign lesions. Based on CESM and CE-MRI, 4 false-positive cases and 3 false-negative cases and 7 false-positive cases and 1 false-negative case, respectively, were found. The accuracy of CESM was higher than that of MRI (96.3% vs 95.7%), and the specificity was higher than that of MRI (63.6% vs 36.4%). There were no significant differences in the sensitivity, specificity, and accuracy for the detection of MMBC between CESM and CE-MRI (p = 0.500; p = 0.250; p = 0.792).
Conclusion: CESM is an effective method for the detection of MMBC, which is consistent with the sensitivity and accuracy of CE-MRI.
Copyright © 2022 Lei Feng et al.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
Diagnostic Value of Contrast-Enhanced Spectral Mammography in Comparison to Magnetic Resonance Imaging in Breast Lesions.J Comput Assist Tomogr. 2019 Mar/Apr;43(2):245-251. doi: 10.1097/RCT.0000000000000832. J Comput Assist Tomogr. 2019. PMID: 30531546 Free PMC article.
-
The diagnostic performance of CESM and CE-MRI in evaluating the pathological response to neoadjuvant therapy in breast cancer: a systematic review and meta-analysis.Br J Radiol. 2020 Aug;93(1112):20200301. doi: 10.1259/bjr.20200301. Epub 2020 Jul 2. Br J Radiol. 2020. PMID: 32574075 Free PMC article.
-
Contrast-enhanced spectral mammography (CESM) versus breast magnetic resonance imaging (MRI): A retrospective comparison in 66 breast lesions.Diagn Interv Imaging. 2017 Feb;98(2):113-123. doi: 10.1016/j.diii.2016.08.013. Epub 2016 Sep 26. Diagn Interv Imaging. 2017. PMID: 27687829
-
Comparison between breast MRI and contrast-enhanced spectral mammography.Med Sci Monit. 2015 May 12;21:1358-67. doi: 10.12659/MSM.893018. Med Sci Monit. 2015. PMID: 25963880 Free PMC article. Clinical Trial.
-
Angiomammography: A review of current evidences.Diagn Interv Imaging. 2019 Oct;100(10):593-605. doi: 10.1016/j.diii.2019.01.011. Epub 2019 Apr 5. Diagn Interv Imaging. 2019. PMID: 30962168 Review.
Cited by
-
Contrast-enhanced mammography (CEM) versus MRI for breast cancer staging: detection of additional malignant lesions not seen on conventional imaging.Eur Radiol Exp. 2023 Feb 13;7(1):8. doi: 10.1186/s41747-022-00318-5. Eur Radiol Exp. 2023. PMID: 36781808 Free PMC article. Clinical Trial.
-
Special Issue "New Advances in Breast Imaging".Tomography. 2022 Jun 28;8(4):1702-1703. doi: 10.3390/tomography8040142. Tomography. 2022. PMID: 35894007 Free PMC article.
-
Detection of a contralateral breast malignancy using contrast-enhanced mammography (CEM) overlooked by initial MRI scan.Radiol Case Rep. 2025 Jun 11;20(9):4275-4285. doi: 10.1016/j.radcr.2025.05.046. eCollection 2025 Sep. Radiol Case Rep. 2025. PMID: 40575371 Free PMC article.
-
A case report of breast cancer in silicone-injected breasts diagnosed by an emerging technique of contrast-enhanced mammography-guided biopsy.Front Oncol. 2022 Jul 22;12:884576. doi: 10.3389/fonc.2022.884576. eCollection 2022. Front Oncol. 2022. PMID: 35936726 Free PMC article.
-
Comparative analysis of diagnostic performance of automatic breast ultrasound and spectral mammography as complementary methods to mammography examination.Pol J Radiol. 2025 Feb 3;90:e55-e65. doi: 10.5114/pjr/199755. eCollection 2025. Pol J Radiol. 2025. PMID: 40196314 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
