

The disconnect between visual assessment of air trapping and lung physiology for assessment of small airway disease in scleroderma-related interstitial lung disease: An observation from the Scleroderma Lung Study II Cohort
- PMID: 35585954
- PMCID: PMC9109505
- DOI: 10.1177/23971983211047160
The disconnect between visual assessment of air trapping and lung physiology for assessment of small airway disease in scleroderma-related interstitial lung disease: An observation from the Scleroderma Lung Study II Cohort
Abstract
Objective: To explore the presence of small airway disease (SAD) and emphysema in scleroderma-related interstitial lung disease (SSc-ILD) and to evaluate the physiologic and clinical correlates of SAD in SSc-ILD.
Methods: Thoracic high-resolution computed tomography (HRCT) images obtained from the Scleroderma Lung Study II (SLSII) participants were reviewed by a group of thoracic radiologists. The presence of SAD was assessed by visual assessment for air trapping. HRCT scans were also evaluated for the presence of emphysema. The association of the presence of air trapping and emphysema with physiological measures of airway disease and clinical variables was evaluated.
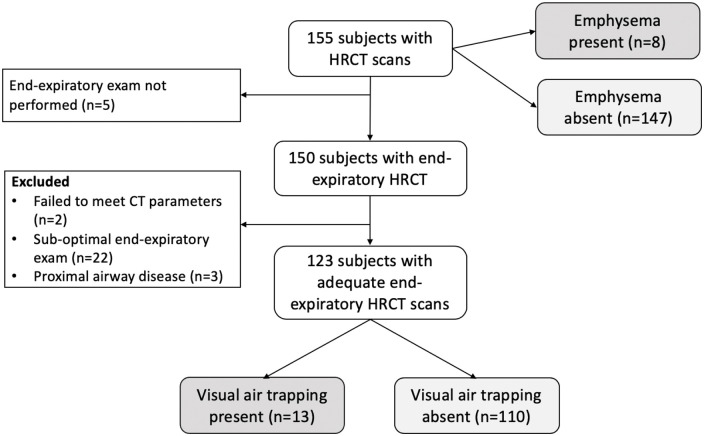
Results: A total of 155 baseline HRCT scans were reviewed. For assessment of air trapping, images needed to be adequate end-expiratory examinations, leaving 123 scans. Air trapping was seen in 13/123 (10.6%) of the SSc-ILD cohort and was independent of smoking history, asthma or the presence of gastroesophageal reflux. Air trapping on HRCT was not associated with physiologic evidence of SAD. We also identified 8/155 (5.2%) patients with emphysema on HRCT, which was independent of SAD and found mostly in prior smokers.
Conclusion: We report the first study of air trapping on standardized, high-quality HRCT images as a reflection of SAD in a relatively large, well characterized SSc-ILD cohort. The presence of SAD in non-smoking SSc-ILD patients supports that SSc may cause not only restrictive lung disease (SSc-ILD), but also, to a lesser extent, obstructive disease. Physiologic measures alone may be inadequate to detect airway disease in patients with SSc-ILD.
Keywords: Scleroderma; air trapping; emphysema; interstitial lung disease; small airway disease; systemic sclerosis.
© The Author(s) 2021.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Tashkin has served as a consultant in clinical trials funded by Genentech and EMD Serono. Dr. Furst has received research support from Corbus, CSL Behring, Galapagos Gilead, GSK, Kadmon, PICORI, Pfizer, Talaris, and Mitsubishi and serves as a consultant to Abbvie, Corbus, Galapagos, Gilead, Novartis, Pfizer, Talaris, R-Pharm, CSL Behring, and Boehringer Ingelheim. There was no conflict of interest for all authors.
Figures
Similar articles
-
Prevalence and clinical correlates of small airway obstruction in patients with systemic sclerosis.Clin Rheumatol. 2021 Apr;40(4):1417-1422. doi: 10.1007/s10067-020-05353-4. Epub 2020 Aug 22. Clin Rheumatol. 2021. PMID: 32827283
-
Brief Report: Pulmonary Function Tests: High Rate of False-Negative Results in the Early Detection and Screening of Scleroderma-Related Interstitial Lung Disease.Arthritis Rheumatol. 2015 Dec;67(12):3256-61. doi: 10.1002/art.39405. Arthritis Rheumatol. 2015. PMID: 26316389
-
Clinical algorithms for the diagnosis and prognosis of interstitial lung disease in systemic sclerosis.Semin Arthritis Rheum. 2017 Oct;47(2):228-234. doi: 10.1016/j.semarthrit.2017.03.019. Epub 2017 Apr 1. Semin Arthritis Rheum. 2017. PMID: 28454677
-
Predictors of progression in systemic sclerosis patients with interstitial lung disease.Eur Respir J. 2020 May 14;55(5):1902026. doi: 10.1183/13993003.02026-2019. Print 2020 May. Eur Respir J. 2020. PMID: 32079645 Free PMC article. Review.
-
Gastroesophageal reflux incites interstitial lung disease in systemic sclerosis: clinical, radiologic, histopathologic, and treatment evidence.Semin Arthritis Rheum. 2010 Dec;40(3):241-9. doi: 10.1016/j.semarthrit.2010.03.002. Epub 2010 May 21. Semin Arthritis Rheum. 2010. PMID: 20494406 Review.
Cited by
-
Syndrome of Combined Pulmonary Fibrosis and Emphysema: An Official ATS/ERS/JRS/ALAT Research Statement.Am J Respir Crit Care Med. 2022 Aug 15;206(4):e7-e41. doi: 10.1164/rccm.202206-1041ST. Am J Respir Crit Care Med. 2022. PMID: 35969190 Free PMC article.
References
-
- Rubio-Rivas M, Royo C, Simeon CP, et al.. Mortality and survival in systemic sclerosis: systematic review and meta-analysis. Semin Arthritis Rheum 2014; 44(2): 208–219. - PubMed
-
- D’Angelo WA, Fries JF, Masi AT, et al.. Pathologic observations in systemic sclerosis (scleroderma). Am J Med 1969; 46(3): 428–440. - PubMed
-
- Weaver AL, Divertie MB, Titus JL. Pulmonary scleroderma. Dis Chest 1968; 54: 490–498. - PubMed
-
- Bjerke RD, Tashkin DP, Clements PJ, et al.. Small airways in progressive systemic sclerosis (PSS). Am J Med 1979; 66: 201–209. - PubMed
-
- Guttadauria M, Ellman H, Emmanuel G, et al.. Pulmonary function in scleroderma. Arthritis Rheum 1977; 20: 1071–1079. - PubMed