

The First Case Report of Preschool-Onset SS/SLE Coexisting With NMOSD of Chinese Origin
- PMID: 35585974
- PMCID: PMC9108358
- DOI: 10.3389/fimmu.2022.887041
The First Case Report of Preschool-Onset SS/SLE Coexisting With NMOSD of Chinese Origin
Abstract
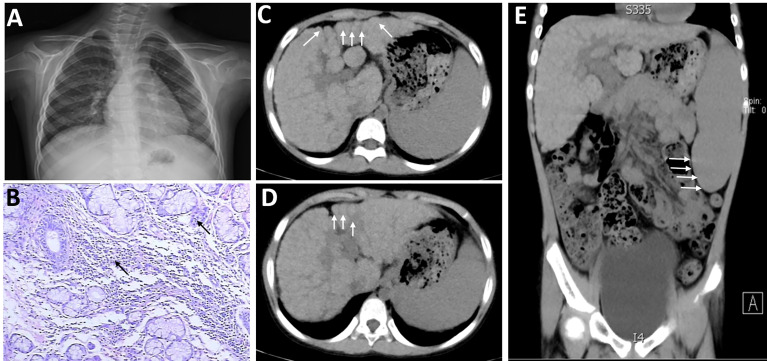
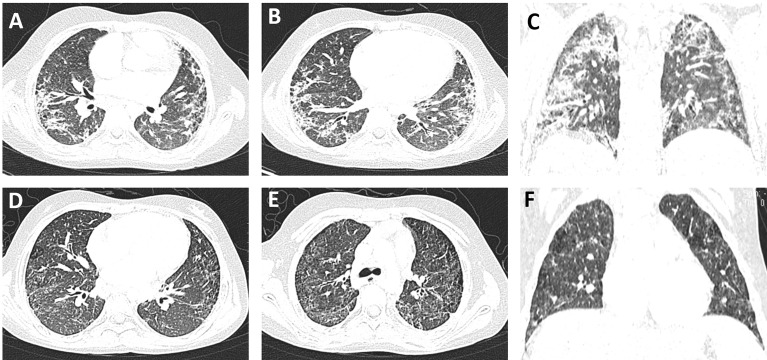
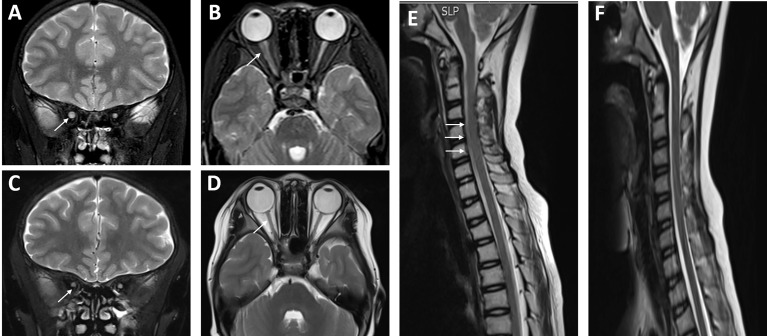
Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease (CTD), the main features of which are multiple serum autoantibodies and extensive involvement of multiple systems. The onset age of patients varies from childhood to middle age, with nearly 1/5 in childhood. Sjogren's syndrome (SS) is also an autoimmune disease characterized by high-degree lymphocytic infiltration of exocrine glands, usually occurring in middle-aged and older women, and rarely in childhood. Neuromyelitis optica spectrum disorder (NMOSD) is an immune-mediated inflammatory demyelinating disease of the central nervous system (CNS) mainly involving the optic nerve and spinal cord. The coexistence of NMOSD and SLE and/or SS is well recognized by both neurologists and rheumatologists, but cases in children have been rarely reported. In this paper, we reported a case of a girl with onset at age 5 clinically featured by recurrent parotid gland enlargement, pancytopenia, hypocomplementemia, multiple positive serum antibodies, and cirrhosis. She was initially diagnosed with SS/SLE overlap syndrome at age 5. Four years later, the patient suffered a sudden vision loss and was examined to have positive AQP4 antibodies in serum and cerebrospinal fluid (CSF), and long segmental spinal swelling, in line with the diagnostic criteria for NMOSD. Up to now, the current patient is of the youngest onset age to develop SS/SLE coexisting with NMOSD, also with cirrhosis. It is important for clinicians to be aware of the possibility of CTDs coexisting with NMOSD in children, especially in those with positive anti-multiple autoantibodies, and to decrease the rate of missed diagnosis.
Keywords: AQP-4; Sjogren’s syndrome; child SS/SLE overlap syndrome with NMOSD; neuromyelitis optica spectrum disorder; systemic lupus erythematosus.
Copyright © 2022 Liu, Tang, Zhang, Li, Huang, Xiong, Xiao and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A Chinese girl with neuromyelitis optica spectrum disorder coexisting with primary Sjogren's syndrome: a case report and literature review.Front Immunol. 2025 Jul 8;16:1559825. doi: 10.3389/fimmu.2025.1559825. eCollection 2025. Front Immunol. 2025. PMID: 40698091 Free PMC article. Review.
-
Neuromyelitis Optica Spectrum Disorders (NMOSD) and Connective Tissue Disease (CTD): an Update for the Rheumatologist.Curr Rheumatol Rep. 2021 Apr 28;23(6):33. doi: 10.1007/s11926-021-01000-2. Curr Rheumatol Rep. 2021. PMID: 33909180 Review.
-
Seropositive Neuromyelitis Optica in a Case of Undiagnosed Ankylosing Spondylitis: A Neuro-Rheumatological Conundrum.Qatar Med J. 2022 Jul 7;2022(3):29. doi: 10.5339/qmj.2022.29. eCollection 2022. Qatar Med J. 2022. PMID: 35864917 Free PMC article.
-
A novel association of osmotic demyelination in Sjögren's syndrome prompts revisiting role of aquaporins in CNS demyelinating diseases: A literature review.Mult Scler Relat Disord. 2023 Jan;69:104466. doi: 10.1016/j.msard.2022.104466. Epub 2022 Dec 11. Mult Scler Relat Disord. 2023. PMID: 36584554 Review.
-
Overlap syndrome of anti-aquaporin-4 positive neuromyelitis optica spectrum disorder and systemic lupus erythematosus: A systematic review of individual patient data.Lupus. 2023 Sep;32(10):1164-1172. doi: 10.1177/09612033231191180. Epub 2023 Jul 24. Lupus. 2023. PMID: 37487596
Cited by
-
Spectrum of Central Nervous System Involvement in Childhood-Onset Sjögren's Syndrome: A Case-Based Review.Mediterr J Rheumatol. 2024 May 21;35(2):298-304. doi: 10.31138/mjr.241123.soc. eCollection 2024 Jun. Mediterr J Rheumatol. 2024. PMID: 39211020 Free PMC article.
-
A Chinese child with both systemic lupus erythematosus coexisting with neuromyelitis optica spectrum disorder: a case report.Pediatr Rheumatol Online J. 2024 Dec 18;22(1):107. doi: 10.1186/s12969-024-01045-4. Pediatr Rheumatol Online J. 2024. PMID: 39695852 Free PMC article. No abstract available.
-
A case report of AQP4-IgG-seropositive refractory neuromyelitis optica spectrum disorder patient with Sjögren's syndrome and pancytopenia treated with inebilizumab.Front Neurol. 2024 Jun 5;15:1371515. doi: 10.3389/fneur.2024.1371515. eCollection 2024. Front Neurol. 2024. PMID: 38899058 Free PMC article.
-
A Chinese girl with neuromyelitis optica spectrum disorder coexisting with primary Sjogren's syndrome: a case report and literature review.Front Immunol. 2025 Jul 8;16:1559825. doi: 10.3389/fimmu.2025.1559825. eCollection 2025. Front Immunol. 2025. PMID: 40698091 Free PMC article. Review.
-
[Diagnostic value of low versus high titers of MOG-IgG and their clinical implications in myelin oligodendrocyte glycoprotein antibody-associated disease: a retrospective singlecenter study].Nan Fang Yi Ke Da Xue Xue Bao. 2023 Nov 20;43(11):1865-1873. doi: 10.12122/j.issn.1673-4254.2023.11.05. Nan Fang Yi Ke Da Xue Xue Bao. 2023. PMID: 38081603 Free PMC article. Chinese.
References
-
- Richard C, Ruiz A, Cavagna S, Bigotte M, Vukusic S, Masaki K, et al. . Connexins in Neuromyelitis Optica: A Link Between Astrocytopathy and Demyelination. Brain (2020) 143(9):2721–32. doi: 10.1093/brain/awaa227 - DOI
-
- Jarius S, Wildemann B. AQP4 Antibodies in Neuromyelitis Optica: Diagnostic and Pathogenetic Relevance. Nat Rev Neurol (2010) 6(7):383–92. doi: 10.1038/nrneurol.2010.72 - DOI
-
- Jarius S, Jacobi C, de Seze J, Zephir H, Paul F, Franciotta D, et al. . Frequency and Syndrome Specificity of Antibodies to Aquaporin-4 in Neurological Patients With Rheumatic Disorders. Mult Scler (2011) 17(9):1067–73. doi: 10.1177/1352458511403958 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical