

Association Between Serum Sodium and Long-Term Mortality in Critically Ill Patients with Comorbid Chronic Obstructive Pulmonary Disease: Analysis from the MIMIC-IV Database
- PMID: 35586119
- PMCID: PMC9112792
- DOI: 10.2147/COPD.S353741
Association Between Serum Sodium and Long-Term Mortality in Critically Ill Patients with Comorbid Chronic Obstructive Pulmonary Disease: Analysis from the MIMIC-IV Database
Abstract
Purpose: The purpose of our study was to investigate the relationship between serum sodium levels and 1-year and 3-year mortality in critically ill patients with comorbid chronic obstructive pulmonary disease using real-world data.
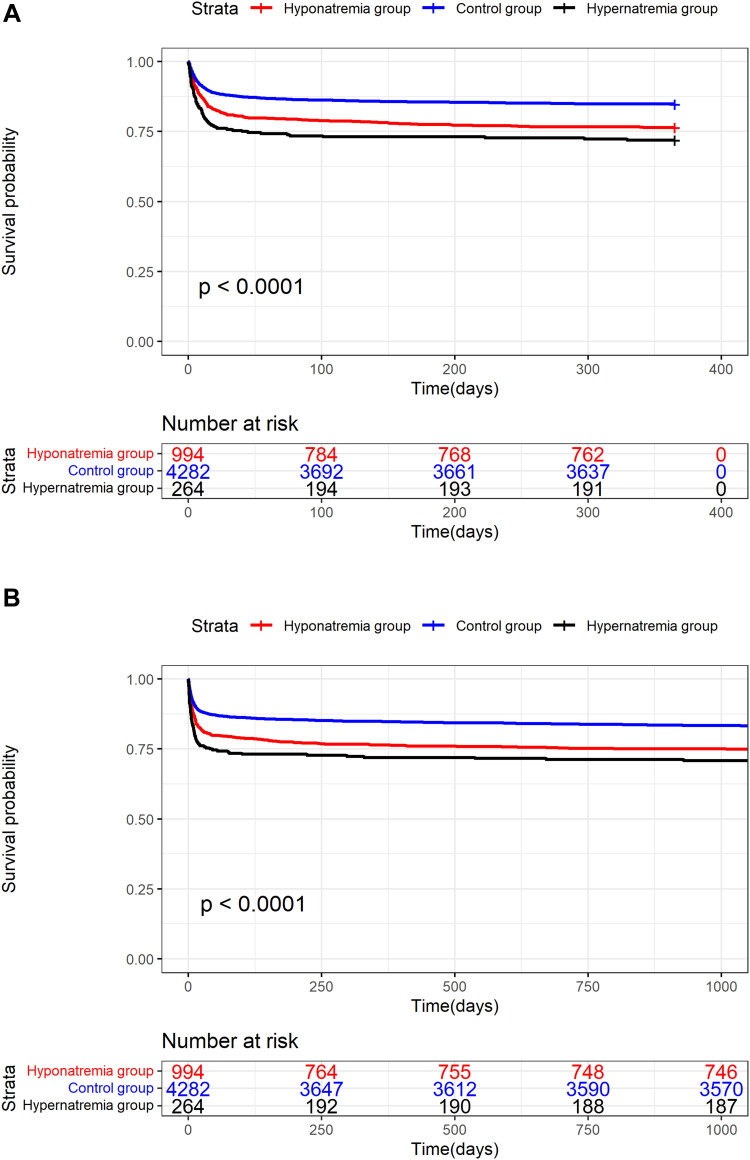
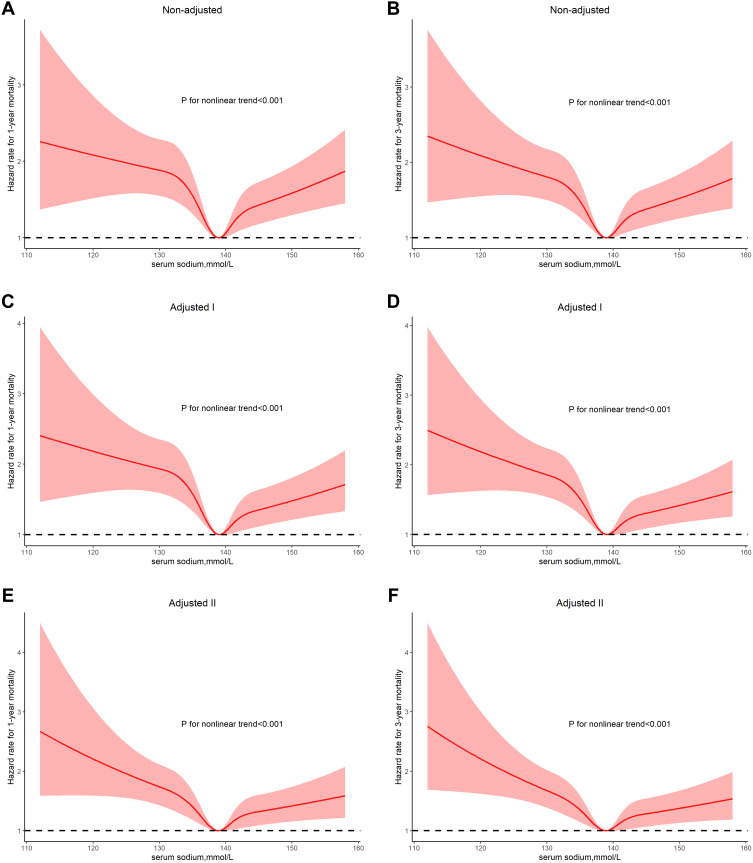
Methods: The data of this study were collected from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database. First of all, we used the Kaplan-Meier curves and multivariable Cox regression analyses to measure the relationship between serum sodium levels and 1-year and 3-year mortality for critically ill patients with comorbid COPD. Next, a restricted cubic spline was used to analyze non-parametrically the relationship between mortality and serum sodium as a continuous variable. In addition, we also analyzed the mortality of different subgroups.
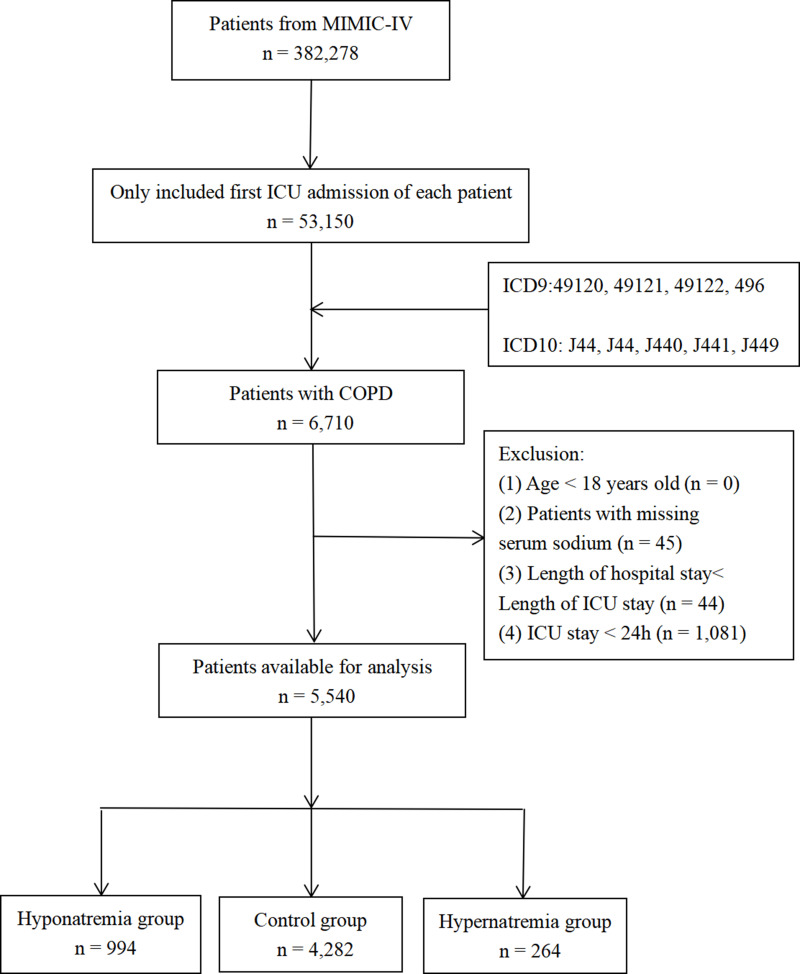
Results: A total of 5540 eligible subjects were extracted. Compared to normal serum sodium levels, adjusted multivariable Cox regression analysis confirmed that hyponatremia and hypernatremia were still significantly associated with 1-year mortality (HR = 1.551, 95% CI = 1.333~1.805, P<0.001; HR = 1.683, 95% CI = 1.317~2.151, P<0.001, respectively) and 3-year mortality (HR = 1.507, 95% CI = 1.302~1.744, P<0.001; HR = 1.612, 95% CI = 1.269~2.048, P<0.001, respectively). In patients with or without adjustment variables, there was an obvious U-shaped non-linear relationship between serum sodium levels and 1-year and 3-year mortality with a reference level of 139 mmol/L, which indicated that patients in both hyponatremia and hypernatremia had higher mortality than normal serum sodium levels.
Conclusion: This study showed that both hyponatremia and hypernatremia were related to increased 1-year and 3-year mortality in critically ill patients with comorbid COPD, which provides a new reference for the control strategy of correcting serum sodium levels.
Keywords: MIMIC-IV; chronic obstructive pulmonary disease; intensive care unit; serum sodium.
© 2022 Fan et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Association between serum sodium level trajectories and survival in patients with heart failure.ESC Heart Fail. 2023 Feb;10(1):255-263. doi: 10.1002/ehf2.14187. Epub 2022 Oct 3. ESC Heart Fail. 2023. PMID: 36193558 Free PMC article.
-
Abnormal Serum Sodium is Associated With Increased Mortality Among Unselected Cardiac Intensive Care Unit Patients.J Am Heart Assoc. 2020 Jan 21;9(2):e014140. doi: 10.1161/JAHA.119.014140. Epub 2020 Jan 9. J Am Heart Assoc. 2020. PMID: 31914877 Free PMC article.
-
Prognostic consequences of borderline dysnatremia: pay attention to minimal serum sodium change.Crit Care. 2013 Jan 21;17(1):R12. doi: 10.1186/cc11937. Crit Care. 2013. PMID: 23336363 Free PMC article.
-
Neurologic Intensive Care Unit Electrolyte Management.Nurs Clin North Am. 2017 Jun;52(2):321-329. doi: 10.1016/j.cnur.2017.01.009. Epub 2017 Apr 7. Nurs Clin North Am. 2017. PMID: 28478880 Review.
-
Association of serum sodium and risk of all-cause mortality in patients with chronic kidney disease: A meta-analysis and sysematic review.Sci Rep. 2017 Nov 21;7(1):15949. doi: 10.1038/s41598-017-16242-3. Sci Rep. 2017. PMID: 29162909 Free PMC article.
Cited by
-
Association between serum sodium levels within 24 h of admission and all-cause mortality in critically ill patients with non-traumatic subarachnoid hemorrhage: a retrospective analysis of the MIMIC-IV database.Front Neurol. 2023 Sep 15;14:1234080. doi: 10.3389/fneur.2023.1234080. eCollection 2023. Front Neurol. 2023. PMID: 37780696 Free PMC article.
-
Relationship Between Systemic Immune-Inflammation Index and Risk of Respiratory Failure and Death in COPD: A Retrospective Cohort Study Based on the MIMIC-IV Database.Int J Chron Obstruct Pulmon Dis. 2024 Feb 19;19:459-473. doi: 10.2147/COPD.S446364. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 38404653 Free PMC article.
-
Association Between the Serum Phosphate Levels and Hospital Mortality as Well as 90-Day Mortality Among Critically Ill Patients with Chronic Obstructive Pulmonary Disease: A Retrospective Cohort Study.Int J Chron Obstruct Pulmon Dis. 2024 Jul 18;19:1681-1693. doi: 10.2147/COPD.S465752. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39055391 Free PMC article.
-
Association Between Geriatric Nutrition Risk Index and 90-Day Mortality in Older Adults with Chronic Obstructive Pulmonary Disease: a Retrospective Cohort Study.Int J Chron Obstruct Pulmon Dis. 2024 May 30;19:1197-1206. doi: 10.2147/COPD.S457422. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 38831891 Free PMC article.
-
Impact of Hyponatraemia at Clinical Stable-State on Survival in Patients with Chronic Obstructive Pulmonary Disease.Int J Chron Obstruct Pulmon Dis. 2025 Jan 15;20:127-135. doi: 10.2147/COPD.S488309. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 39830625 Free PMC article.
References
-
- Soriano JB, Abajobir AA, Abate KH, GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden Of Disease Study 2015. Lancet Respir Med. 2017;5 (9):691–706. - PMC - PubMed
-
- The Lancet Public Health. Ageing: a 21st century public health challenge? Lancet Public Health. 2017;2 (7):e297. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
