

Ovarian stimulation strategies for intrauterine insemination in couples with unexplained infertility: a systematic review and individual participant data meta-analysis
- PMID: 35587030
- PMCID: PMC9434229
- DOI: 10.1093/humupd/dmac021
Ovarian stimulation strategies for intrauterine insemination in couples with unexplained infertility: a systematic review and individual participant data meta-analysis
Abstract
Background: Intrauterine insemination with ovarian stimulation (IUI-OS) is a first-line treatment for unexplained infertility. Gonadotrophins, letrozole and clomiphene citrate (CC) are commonly used agents during IUI-OS and have been compared in multiple aggregate data meta-analyses, with substantial heterogeneity and no analysis on time-to-event outcomes. Individual participant data meta-analysis (IPD-MA) is considered the gold standard for evidence synthesis as it can offset inadequate reporting of individual studies by obtaining the IPD, and allows analyses on treatment-covariate interactions to identify couples who benefit most from a particular treatment.
Objective and rationale: We performed this IPD-MA to compare the effectiveness and safety of ovarian stimulation with gonadotrophins, letrozole and CC and to explore treatment-covariate interactions for important baseline characteristics in couples undergoing IUI.
Search methods: We searched electronic databases including MEDLINE, EMBASE, CENTRAL, CINAHL, and PsycINFO from their inception to 28 June 2021. We included randomized controlled trials (RCTs) comparing IUI-OS with gonadotrophins, letrozole and CC among couples with unexplained infertility. We contacted the authors of eligible RCTs to share the IPD and established the IUI IPD-MA Collaboration. The primary effectiveness outcome was live birth and the primary safety outcome was multiple pregnancy. Secondary outcomes were other reproductive outcomes, including time to conception leading to live birth. We performed a one-stage random effects IPD-MA.
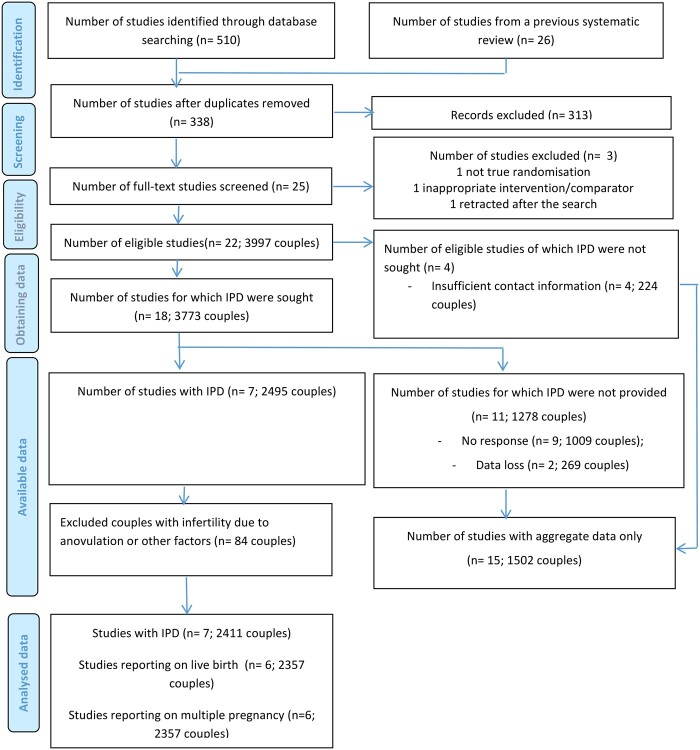
Outcomes: Seven of 22 (31.8%) eligible RCTs provided IPD of 2495 couples (62.4% of the 3997 couples participating in 22 RCTs), of which 2411 had unexplained infertility and were included in this IPD-MA. Six RCTs (n = 1511) compared gonadotrophins with CC, and one (n = 900) compared gonadotrophins, letrozole and CC. Moderate-certainty evidence showed that gonadotrophins increased the live birth rate compared to CC (6 RCTs, 2058 women, RR 1.30, 95% CI 1.12-1.51, I2 = 26%). Low-certainty evidence showed that gonadotrophins may also increase the multiple pregnancy rate compared to CC (6 RCTs, 2058 women, RR 2.17, 95% CI 1.33-3.54, I2 = 69%). Heterogeneity on multiple pregnancy could be explained by differences in gonadotrophin starting dose and choice of cancellation criteria. Post-hoc sensitivity analysis on RCTs with a low starting dose of gonadotrophins (≤75 IU) confirmed increased live birth rates compared to CC (5 RCTs, 1457 women, RR 1.26, 95% CI 1.05-1.51), but analysis on only RCTs with stricter cancellation criteria showed inconclusive evidence on live birth (4 RCTs, 1238 women, RR 1.15, 95% CI 0.94-1.41). For multiple pregnancy, both sensitivity analyses showed inconclusive findings between gonadotrophins and CC (RR 0.94, 95% CI 0.45-1.96; RR 0.81, 95% CI 0.32-2.03, respectively). Moderate certainty evidence showed that gonadotrophins reduced the time to conception leading to a live birth when compared to CC (6 RCTs, 2058 women, HR 1.37, 95% CI 1.15-1.63, I2 = 22%). No strong evidence on the treatment-covariate (female age, BMI or primary versus secondary infertility) interactions was found.
Wider implications: In couples with unexplained infertility undergoing IUI-OS, gonadotrophins increased the chance of a live birth and reduced the time to conception compared to CC, at the cost of a higher multiple pregnancy rate, when not differentiating strategies on cancellation criteria or the starting dose. The treatment effects did not seem to differ in women of different age, BMI or primary versus secondary infertility. In a modern practice where a lower starting dose and stricter cancellation criteria are in place, effectiveness and safety of different agents seem both acceptable, and therefore intervention availability, cost and patients' preferences should factor in the clinical decision-making. As the evidence for comparisons to letrozole is based on one RCT providing IPD, further RCTs comparing letrozole and other interventions for unexplained infertility are needed.
Keywords: clomiphene citrate; gonadotrophins; individual participant data; intrauterine insemination; letrozole; meta-analysis; ovarian stimulation; unexplained infertility.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Figures

References
-
- Al-Fozan H, Al-Khadouri M, Tan SL, Tulandi T.. A randomized trial of letrozole versus clomiphene citrate in women undergoing superovulation. Fertil Steril 2004;82:1561–1563. - PubMed
-
- Badawy A, Elnashar A, Totongy M.. RETRACTED: clomiphene citrate or aromatase inhibitors for superovulation in women with unexplained infertility undergoing intrauterine insemination: a prospective randomized trial. Fertil Steril 2009;92:1355–1359. - PubMed
-
- Balasch J, Ballesca JL, Pimentel C, Creus M, Fabregues F, Vanrell JA.. Late low-dose pure follicle stimulating hormone for ovarian stimulation in intra-uterine insemination cycles. Hum Reprod 1994;9:1863–1866. - PubMed
-
- Baysoy A, Serdaroglu H, Jamal H, Karatekeli E, Ozornek H, Attar E.. Letrozole versus human menopausal gonadotrophin in women undergoing intrauterine insemination. Reprod Biomed Online 2006;13:208–212. - PubMed
-
- Bergh C, Kamath MS, Wang R, Lensen S.. Strategies to reduce multiple pregnancies during medically assisted reproduction. Fertil Steril 2020;114:673–679. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
