

Transfer Patterns of Very Low Birth Weight Infants for Convalescent Care
- PMID: 35588188
- PMCID: PMC9648118
- DOI: 10.1542/peds.2021-054866
Transfer Patterns of Very Low Birth Weight Infants for Convalescent Care
Abstract
Objectives: To examine the prevalence, characteristics, clinical course, and length of stay (LOS) among 4 groups of infants who were transferred for convalescence and subsequently discharged from the hospital; failed transfer for convalescence and were (a) either readmitted, or (b) transferred again; and were not transferred for convalescence.
Methods: Among very low birth weight infants hospitalized at US Vermont Oxford Network centers between 2006 and 2020, we examined the distribution of characteristics, delivery room and NICU usage measures, outcomes, and LOS among the 4 groups of infants.
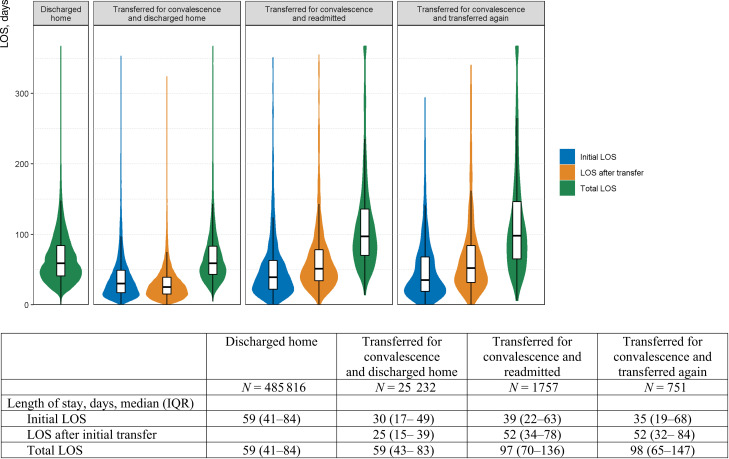
Results: Among 641 712 infants, a total of 28 985 (4.5%) infants were transferred for convalescent care; of 28 186 infants, 182 (0.65%) died before hospital discharge and 2551 (9.1%) failed the transfer (1771 [6.3%] were readmitted and 780 [2.8%] were transferred again). There were major regional and NICU variations in the practice of the transfer for convalescence; New England (18.8%) had the highest whereas East South Central (2.2%) had the lowest percentage of transfer for convalescence. Infants who transferred for convalescence and were discharged from the hospital had a similar LOS and similar distribution of NICU usage measures and outcomes to infants who were not transferred for convalescence. Infants who failed the transfer for convalescence had a longer LOS than infants who were transferred for convalescence and then discharged from the hospital.
Conclusions: The rates of transfer for convalescence and transfer for convalescence failure were low. Future studies should weigh the risks and benefits of transfer for convalescence, which might differ on the basis of geography.
Copyright © 2022 by the American Academy of Pediatrics.
Conflict of interest statement
Figures


Similar articles
-
Convalescent care of infants in the neonatal intensive care unit in community hospitals: risk or benefit?Pediatrics. 2009 Jul;124(1):105-11. doi: 10.1542/peds.2008-0880. Pediatrics. 2009. PMID: 19564289
-
Back transport of neonates: effect on hospital length of stay.J Perinatol. 2005 Nov;25(11):731-6. doi: 10.1038/sj.jp.7211391. J Perinatol. 2005. PMID: 16222344
-
Resource utilization and convalescent care cost in neonatal opioid withdrawal syndrome.J Neonatal Perinatal Med. 2023;16(1):49-57. doi: 10.3233/NPM-221060. J Neonatal Perinatal Med. 2023. PMID: 36530095
-
Pulmonary Support of Infants with Tracheotomies in a Regional Neonatal Intensive Care Unit.Am J Perinatol. 2023 Apr;40(5):539-545. doi: 10.1055/s-0041-1729888. Epub 2021 May 11. Am J Perinatol. 2023. PMID: 33975361 Review.
-
Early NICU discharge of very low birth weight infants: a critical review and analysis.Semin Neonatol. 2003 Apr;8(2):95-115. doi: 10.1016/S1084-2756(02)00219-1. Semin Neonatol. 2003. PMID: 15001147 Review.
Cited by
-
Transfer Patterns Among Infants Born at 28 to 34 Weeks' Gestation.Pediatrics. 2024 Jan 1;153(2):e2023063118. doi: 10.1542/peds.2023-063118. Pediatrics. 2024. PMID: 38268423 Free PMC article.
References
-
- Jung AL, Bose CL. Back transport of neonates: improved efficiency of tertiary nursery bed utilization. Pediatrics. 1983;71(6):918–922 - PubMed
-
- Bose CL, LaPine TR, Jung AL. Neonatal back-transport. Cost-effectiveness. Med Care. 1985;23(1):14–19 - PubMed
-
- Phibbs CS, Mortensen L. Back transporting infants from neonatal intensive care units to community hospitals for recovery care: effect on total hospital charges. Pediatrics. 1992;90(1 Pt 1):22–26 - PubMed
-
- Donohue PK, Hussey-Gardner B, Sulpar LJ, Fox R, Aucott SW. Convalescent care of infants in the neonatal intensive care unit in community hospitals: risk or benefit? Pediatrics. 2009;124(1):105–111 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
