

Clinical Features and Natural History of Preadolescent Nonsyndromic Hypertrophic Cardiomyopathy
- PMID: 35589160
- PMCID: PMC9125690
- DOI: 10.1016/j.jacc.2022.03.347
Clinical Features and Natural History of Preadolescent Nonsyndromic Hypertrophic Cardiomyopathy
Abstract
Background: Up to one-half of childhood sarcomeric hypertrophic cardiomyopathy (HCM) presents before the age of 12 years, but this patient group has not been systematically characterized.
Objectives: The aim of this study was to describe the clinical presentation and natural history of patients presenting with nonsyndromic HCM before the age of 12 years.
Methods: Data from the International Paediatric Hypertrophic Cardiomyopathy Consortium on 639 children diagnosed with HCM younger than 12 years were collected and compared with those from 568 children diagnosed between 12 and 16 years.
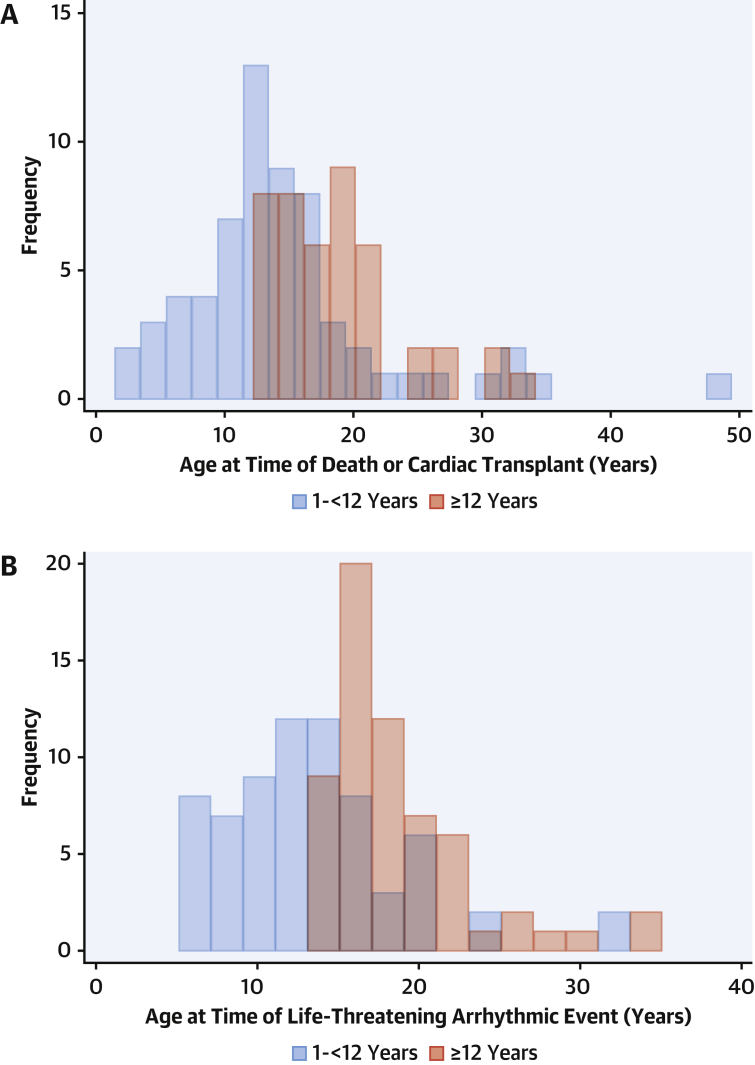
Results: At baseline, 339 patients (53.6%) had family histories of HCM, 132 (20.9%) had heart failure symptoms, and 250 (39.2%) were prescribed cardiac medications. The median maximal left ventricular wall thickness z-score was 8.7 (IQR: 5.3-14.4), and 145 patients (27.2%) had left ventricular outflow tract obstruction. Over a median follow-up period of 5.6 years (IQR: 2.3-10.0 years), 42 patients (6.6%) died, 21 (3.3%) underwent cardiac transplantation, and 69 (10.8%) had life-threatening arrhythmic events. Compared with those presenting after 12 years, a higher proportion of younger patients underwent myectomy (10.5% vs 7.2%; P = 0.045), but fewer received primary prevention implantable cardioverter-defibrillators (18.9% vs 30.1%; P = 0.041). The incidence of mortality or life-threatening arrhythmic events did not differ, but events occurred at a younger age.
Conclusions: Early-onset childhood HCM is associated with a comparable symptom burden and cardiac phenotype as in patients presenting later in childhood. Long-term outcomes including mortality did not differ by age of presentation, but patients presenting at younger than 12 years experienced adverse events at younger ages.
Keywords: age; childhood hypertrophic cardiomyopathy; outcomes; phenotype.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was supported by the British Heart Foundation (grant FS/16/72/32270) to Drs Norrish and Kaski. This work is (partly) funded by the National Institute for Health Research Great Ormond Street Hospital Biomedical Research Centre. Dr Norrish is supported by Great Ormond Street Hospital Children’s Charity. Drs Field and Kaski are supported by Max’s Foundation and Great Ormond Street Hospital Children’s Charity. Dr Kaski is supported by a Medical Research Council–National Institute for Health Research Clinical Academic Research Partnership award. This work was financially supported by the Foundation for Paediatric Research of Finland (Dr Ojala). Dr Fernandez has received speaker fees from Sanofi-Genzyme. Dr Kubus is supported by MH CZ – DRO, Motol University Hospital (00064203). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



Comment in
-
Hypertrophic Cardiomyopathy: A Problem at Any Age.J Am Coll Cardiol. 2022 May 24;79(20):1998-2000. doi: 10.1016/j.jacc.2022.03.356. J Am Coll Cardiol. 2022. PMID: 35589161 No abstract available.
References
-
- Kaski J.P., Syrris P., Esteban M.T., et al. Prevalence of sarcomere protein gene mutations in preadolescent children with hypertrophic cardiomyopathy. Circ Cardiovasc Genet. 2009;2(5):436–441. - PubMed
-
- Maron B.J., Spirito P., Wesley Y., Arce J. Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med. 1986;315(10):610–614. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
