

Worldwide Disparities in Recovery of Cardiac Testing 1 Year Into COVID-19
- PMID: 35589162
- PMCID: PMC9109706
- DOI: 10.1016/j.jacc.2022.03.348
Worldwide Disparities in Recovery of Cardiac Testing 1 Year Into COVID-19
Abstract
Background: The extent to which health care systems have adapted to the COVID-19 pandemic to provide necessary cardiac diagnostic services is unknown.
Objectives: The aim of this study was to determine the impact of the pandemic on cardiac testing practices, volumes and types of diagnostic services, and perceived psychological stress to health care providers worldwide.
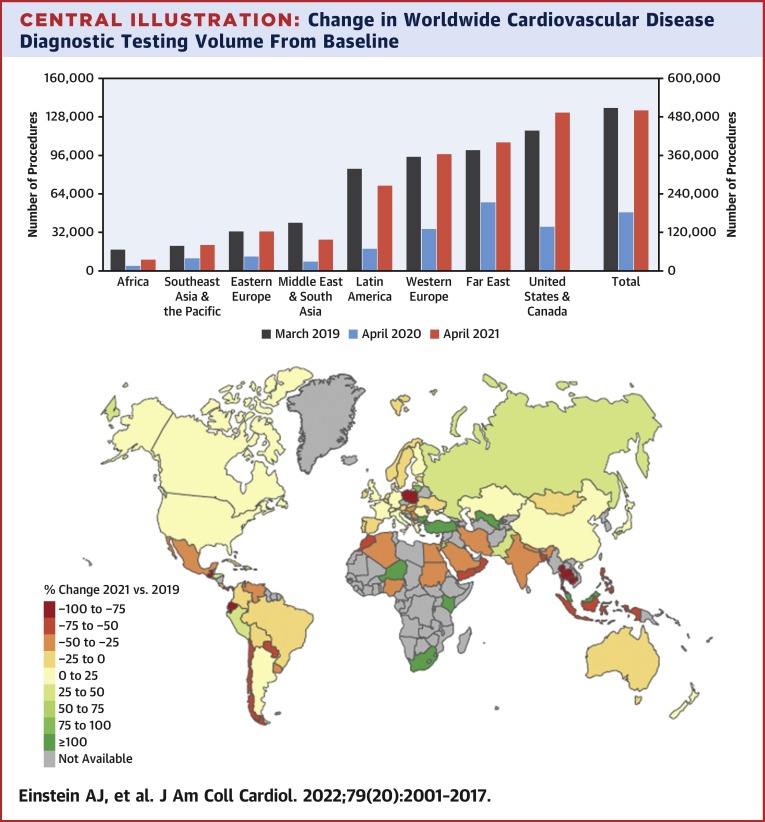
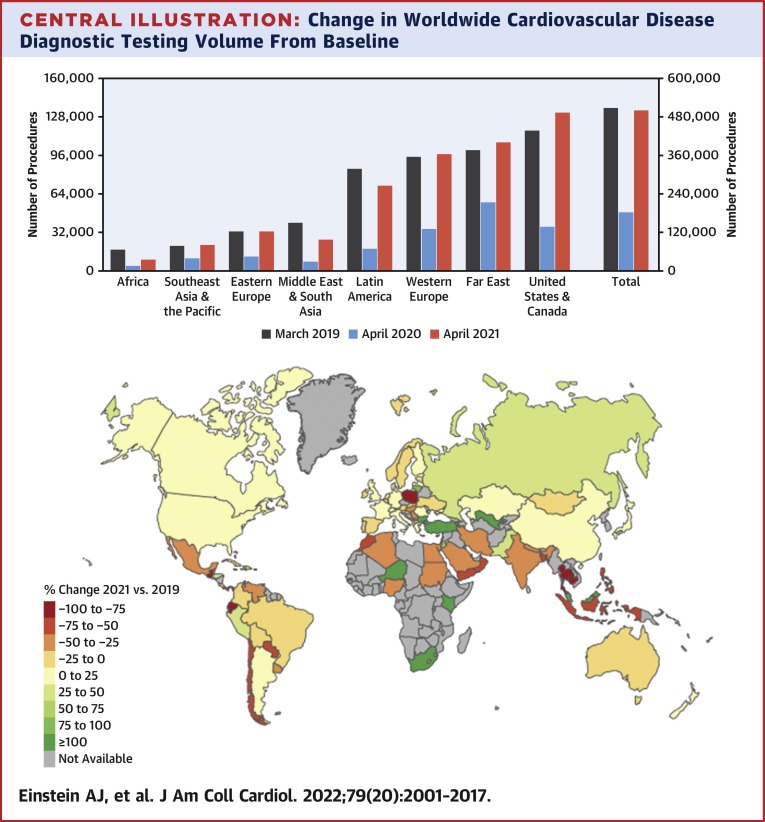
Methods: The International Atomic Energy Agency conducted a worldwide survey assessing alterations from baseline in cardiovascular diagnostic care at the pandemic's onset and 1 year later. Multivariable regression was used to determine factors associated with procedure volume recovery.
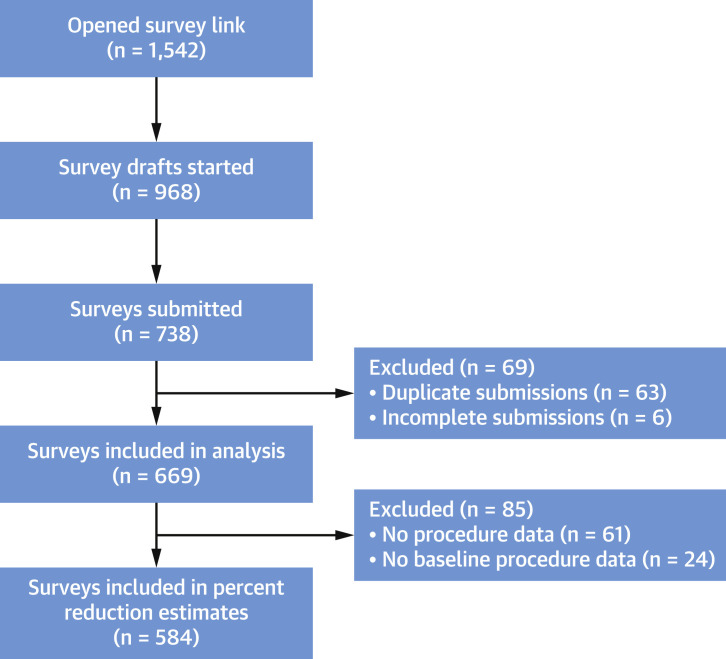
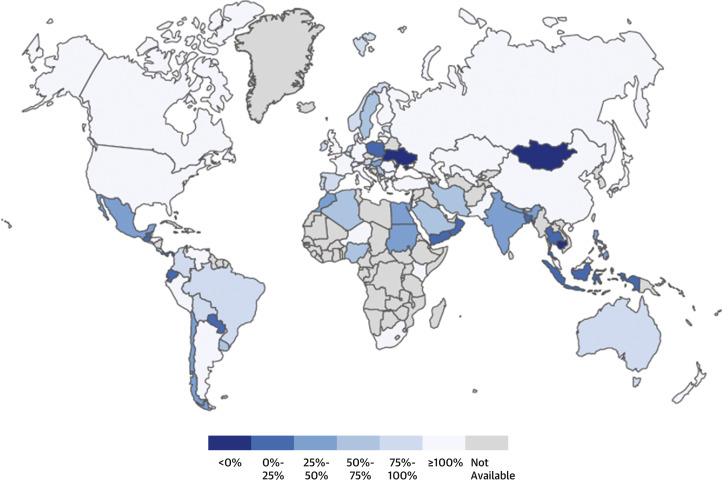
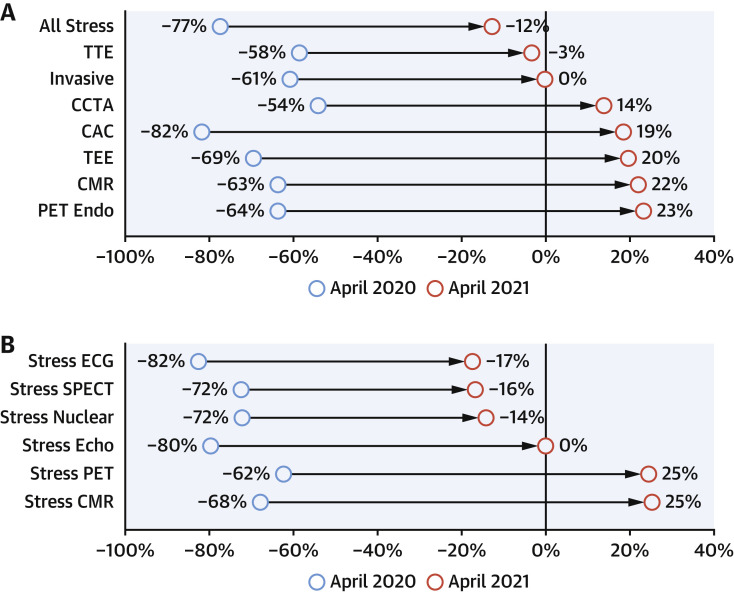
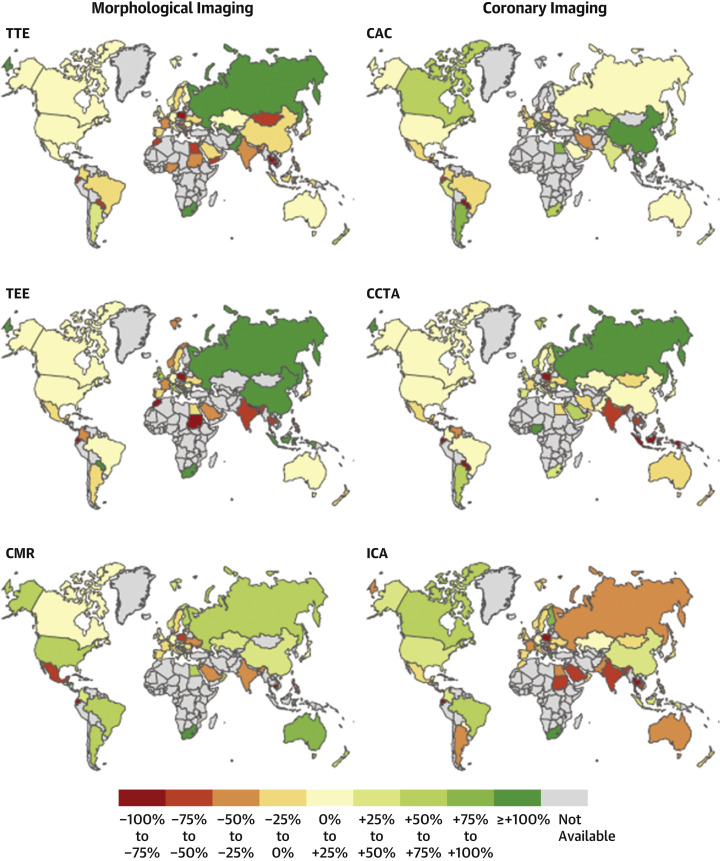
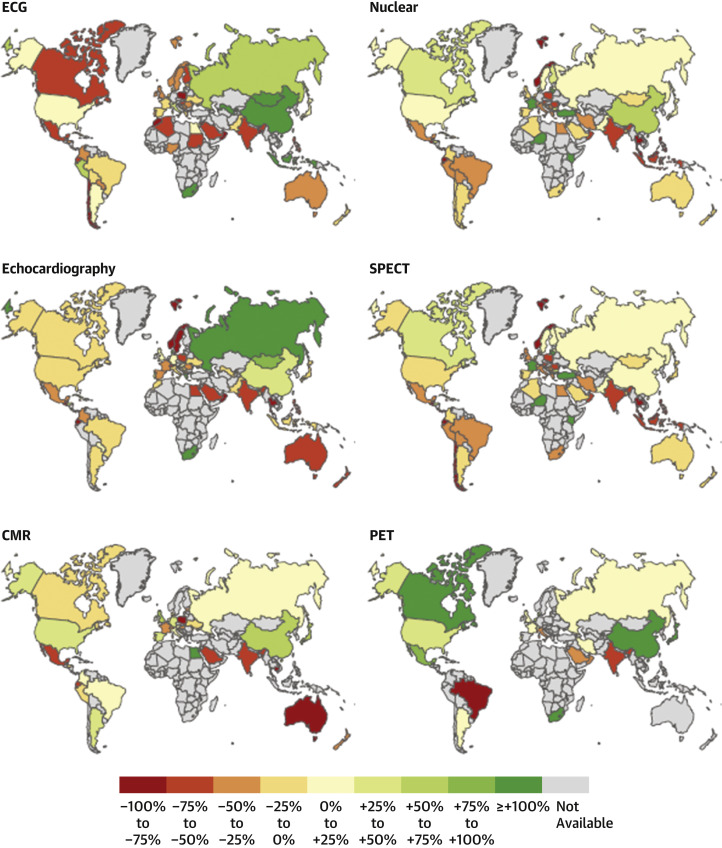
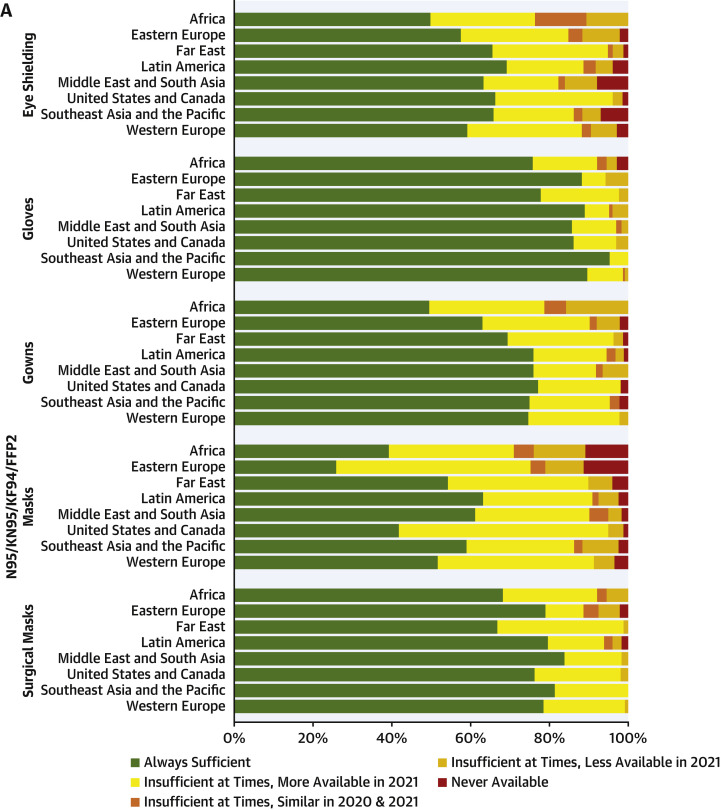
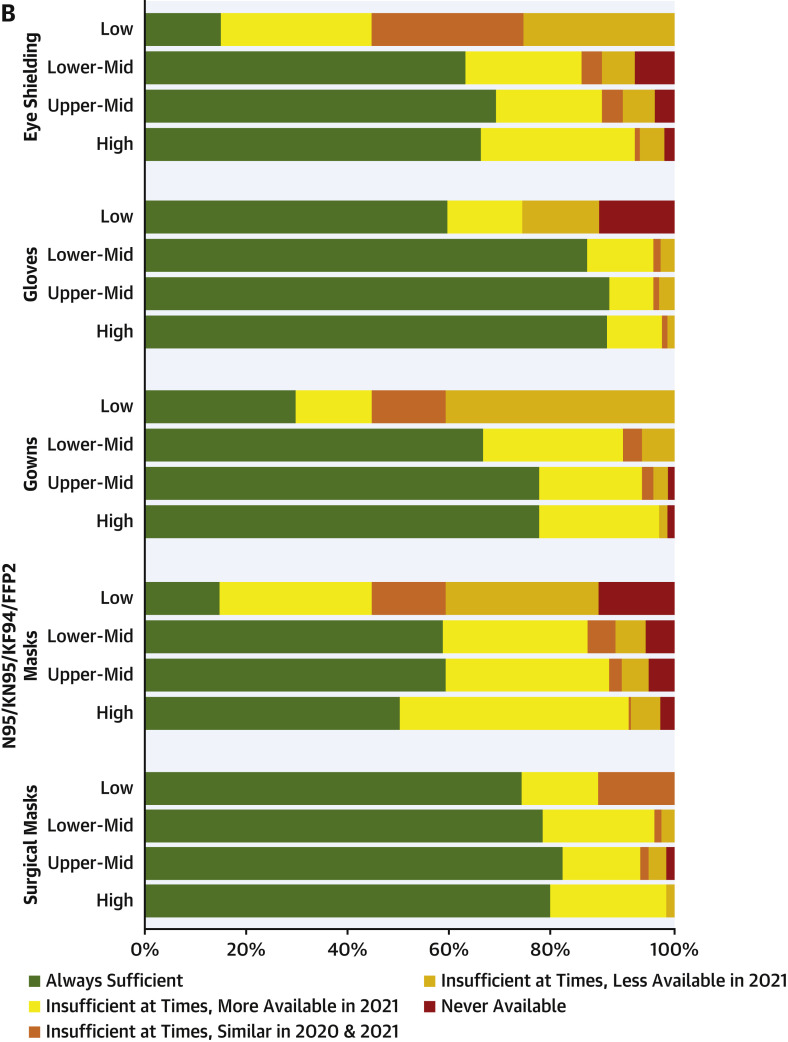
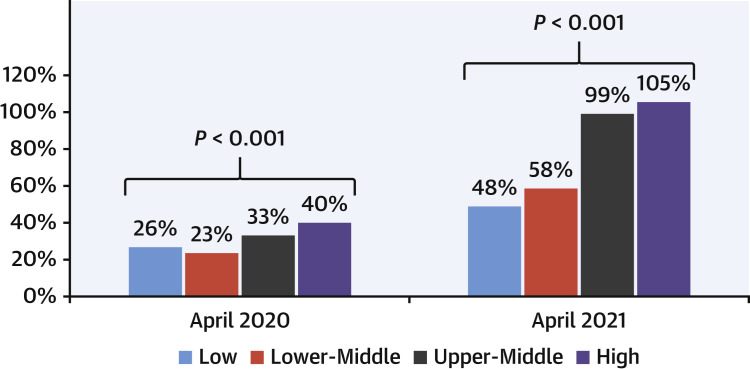
Results: Surveys were submitted from 669 centers in 107 countries. Worldwide reduction in cardiac procedure volumes of 64% from March 2019 to April 2020 recovered by April 2021 in high- and upper middle-income countries (recovery rates of 108% and 99%) but remained depressed in lower middle- and low-income countries (46% and 30% recovery). Although stress testing was used 12% less frequently in 2021 than in 2019, coronary computed tomographic angiography was used 14% more, a trend also seen for other advanced cardiac imaging modalities (positron emission tomography and magnetic resonance; 22%-25% increases). Pandemic-related psychological stress was estimated to have affected nearly 40% of staff, impacting patient care at 78% of sites. In multivariable regression, only lower-income status and physicians' psychological stress were significant in predicting recovery of cardiac testing.
Conclusions: Cardiac diagnostic testing has yet to recover to prepandemic levels in lower-income countries. Worldwide, the decrease in standard stress testing is offset by greater use of advanced cardiac imaging modalities. Pandemic-related psychological stress among providers is widespread and associated with poor recovery of cardiac testing.
Keywords: COVID-19; cardiac testing; cardiovascular disease; coronavirus; global health.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Williams is supported by the British Heart Foundation (FS/ICRF/20/26002). Dr Einstein has received speaker fees from Ionetix; has received consulting fees from W. L. Gore & Associates; has received authorship fees from Wolters Kluwer Healthcare – UpToDate; and has received grants or grants pending to his institution from Attralus, Canon Medical Systems, Eidos Therapeutics, GE Healthcare, Pfizer, Roche Medical Systems, W. L. Gore & Associates, and XyloCor Therapeutics. Dr Williams has received speaker fees from Canon Medical Systems. Dr Dorbala has received honoraria from Pfizer and GE Healthcare; and has received grants to her institution from Pfizer and GE Healthcare. Dr Sinitsyn has received congress speaker honoraria from Bayer, GE Healthcare, Siemens, and Philips. Dr Kudo has received research grants from Nihon Medi-physics and FUJIFILM Toyama Chemical. Dr Bucciarelli-Ducci is CEO (part-time) of the Society for Cardiovascular Magnetic Resonance; and has received speaker fees from Circle Cardiovascular Imaging, Bayer, and Siemens Healthineers. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Unbiased COVID-19 Pandemic With Biased Global Recovery.J Am Coll Cardiol. 2022 May 24;79(20):2018-2020. doi: 10.1016/j.jacc.2022.03.350. J Am Coll Cardiol. 2022. PMID: 35589163 Free PMC article.
References
-
- World Bank Data Team World Bank country and lending groups. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-b... Available at:
-
- Mathieu E., Ritchie H., Ortiz-Ospina E., et al. A global database of COVID-19 vaccinations. Nat Hum Behav. 2021;5:947–953. - PubMed
-
- United Nations UN/DESA Policy Brief #81: impact of COVID-19 on SDG progress: a statistical perspective. https://www.un.org/development/desa/dpad/publication/un-desa-policy-brie... Available at:
