

Grading scale based on arcuate fasciculus segmentation to predict postoperative language outcomes of brain arteriovenous malformations
- PMID: 35589330
- PMCID: PMC9614134
- DOI: 10.1136/svn-2021-001330
Grading scale based on arcuate fasciculus segmentation to predict postoperative language outcomes of brain arteriovenous malformations
Abstract
Objective: The long-term postoperative language outcomes for brain arteriovenous malformations (bAVMs) have not been well characterised. With fibres scattered in the Broca's, Wernicke's and Geschwind's area, the arcuate fasciculus (AF) is considered as a crucial structure of language function. This study aimed to observe the language outcomes, determine the risk factors and construct a grading system for long-term postoperative language deficits (LDs) in patients with bAVMs involving the AF (AF-bAVMs).
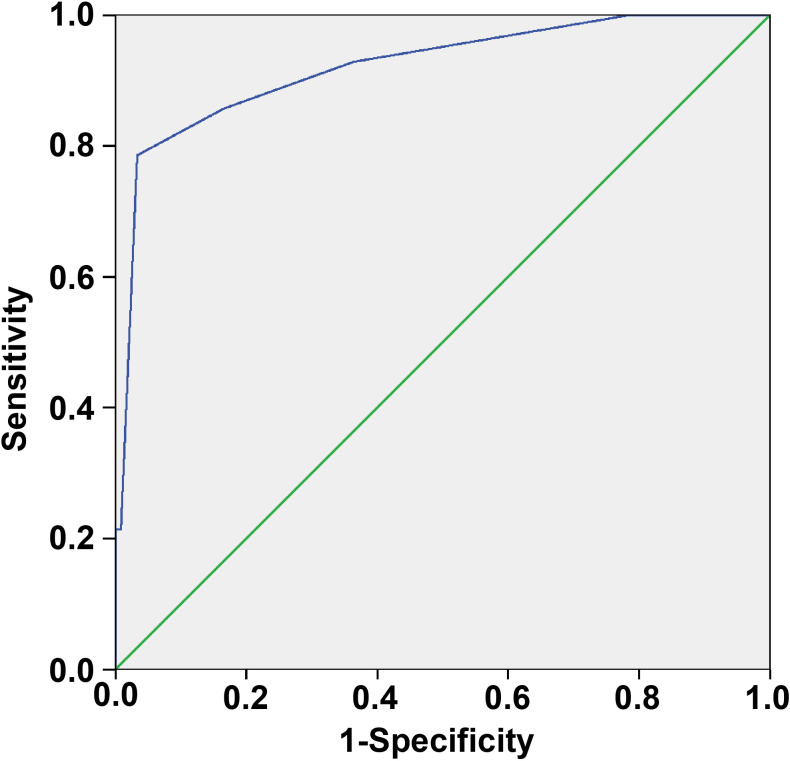
Methods: We retrospectively reviewed 135 patients with AF-bAVMs. Based on the course of the AF and our clinical experience, three boundary lines were drawn to divide the AF into segments I, II, III and IV in spatial order from the frontal lobe to the temporal lobe. Surgery-related LD evaluations were performed 1 week (short term) and at the last follow-up (long term) after surgery. Finally, based on multivariable logistic regression analysis, a grading system was constructed to predict long-term postoperative LD. The predictive accuracy was assessed using the area under the receiver operating characteristic curve (AUC).
Results: Sixty-two (45.9%) patients experienced short-term postoperative LD. After a mean follow-up of 50.2±24.9 months, long-term LD was found in 14 (10.4%) patients. Nidus size (p=0.007), LD history (p=0.009) and segment II involvement (p=0.030) were independent risk factors for short-term LD. Furthermore, segment II involvement (p=0.002), anterior choroidal artery (AChA) feeding (p=0.001), patient age (p=0.023) and LD history (p=0.001) were independent risk factors for long-term LD. A grading system was developed by combining the risk factors for long-term LD; its predictive accuracy was 0.921.
Conclusions: The involvement of the trunk of the AF between Broca's area and the inferior parietal lobule, a nidus supplied by the AChA, older patient age and history of LD were associated with long-term postoperative LD. The grading system combining these factors demonstrated favourable predictive accuracy for long-term language outcomes.
Keywords: Arteriovenous Malformations.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials