

Age-period-cohort analysis of lung cancer mortality in China and Australia from 1990 to 2019
- PMID: 35589955
- PMCID: PMC9120450
- DOI: 10.1038/s41598-022-12483-z
Age-period-cohort analysis of lung cancer mortality in China and Australia from 1990 to 2019
Abstract
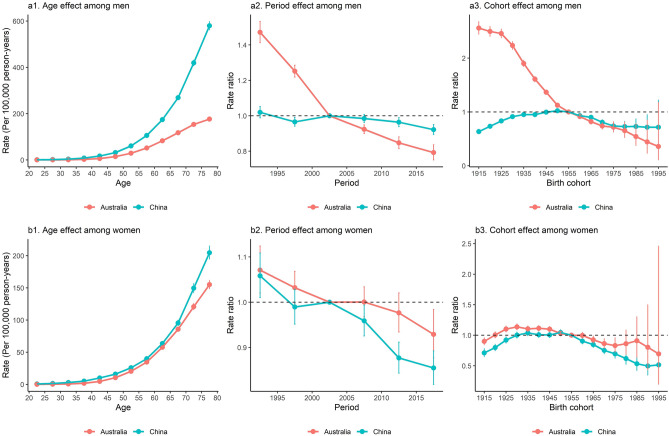
Lung cancer (LC) is the leading cause of cancer death in China and Australia, the countries with different socioenvironmental contexts in the Western Pacific Region. Comparing the age-period-cohort effect on LC mortality (LCM) between the two countries can help plan interventions and draw lessons for countries in the region. We collected LCM estimates between 1990 and 2019 from the GBD 2019. Age-period-cohort modelling was applied to compute the net drift, local drift, cross-sectional age curve, longitudinal age curve, and the rate ratios (RRs) of period and cohort. China had a higher LC age-standardized mortality rate than Australia in 2019 (men: 58.10 [95% uncertainty interval (UI): 46.53, 70.89] vs. 30.13 [95% UI: 27.88, 32.31]/100,000 population; women: 22.86 [95% UI: 18.52, 27.52] vs. 17.80 [95% UI: 15.93, 19.34]/100,000 population). Period and cohort effects on LCM improved more markedly among Australian men (RR for period effect, from 1.47 [95% confidence interval (CI) 1.41, 1.53] to 0.79 [95% CI 0.75, 0.84]; RR for cohort effect, from 2.56 [95% CI 2.44, 2.68] to 0.36 [95% CI 0.11, 1.18]) and Chinese women (RR for period effect, from 1.06 [95% CI 1.01, 1.11] to 0.85 [95% CI 0.82, 0.89]; RR for cohort effect, from 0.71 [95% CI 0.65, 0.78] to 0.51 [95% CI 0.26, 1.03]) during the study period and birth cohort. The LCM in Chinese population aged 65 to 79 and Australian women aged 75 to 79 increased. Smoking and particulate matter (PM) contributed most to LCM in China, while smoking and occupational carcinogens contributed most in Australia. Decreasing period and cohort risks for LCM attributable to smoking and PM were more remarkable in Australia than in China. The LCM attributable to occupational carcinogens was higher in Australia than in China, particularly for those aged 60 to 79. Vigorous tobacco and PM control, which brought a substantial decline in LCM in Australia, may help reduce LCM in China. Australia should highlight LC prevention among people with occupational exposure. Chinese aged ≥ 65 and Australian women aged ≥ 75 should be the priorities for LC interventions.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- World Health Organization. Global NCD Action Plan 2013–2020 (World Health Organization, 2013). https://www.unscn.org/en/news-events/recent-news?idnews=1420.
-
- United Nations. Sustainable Development Goal 3: Ensure Healthy Lives and Promote Well-Being for All at All Ages (United Nations, 2016). https://sustainabledevelopment.un.org/sdg3#targets.
-
- Global Burden of Disease Cancer Collaboration Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 2019;5:1749–1768. doi: 10.1001/jamaoncol.2019.2996. - DOI - PMC - PubMed
-
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2021: Addressing New and Emerging Products (World Health Organization, 2021). https://www.who.int/publications/i/item/9789240032095.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
