

Surgeons' physical workload in open surgery versus robot-assisted surgery and nonsurgical tasks
- PMID: 35589973
- PMCID: PMC9613719
- DOI: 10.1007/s00464-022-09256-0
Surgeons' physical workload in open surgery versus robot-assisted surgery and nonsurgical tasks
Abstract
Background: Musculoskeletal disorders (MSDs) are common among surgeons, and its prevalence varies among surgical modalities. There are conflicting results concerning the correlation between adverse work exposures and MSD prevalence in different surgical modalities. The progress of rationalization in health care may lead to job intensification for surgeons, but the literature is scarce regarding to what extent such intensification influences the physical workload in surgery. The objectives of this study were to quantify the physical workload in open surgery and compare it to that in (1) nonsurgical tasks and (2) two surgeon roles in robot-assisted surgery (RAS).
Methods: The physical workload of 22 surgeons (12 performing open surgery and 10 RAS) was measured during surgical workdays, which includes trapezius muscle activity from electromyography, and posture and movement of the head, upper arms and trunk from inertial measurement units. The physical workload of surgeons in open surgery was compared to that in nonsurgical tasks, and to the chief and assistant surgeons in RAS, and to the corresponding proposed action levels. Mixed-effects models were used to analyze the differences.
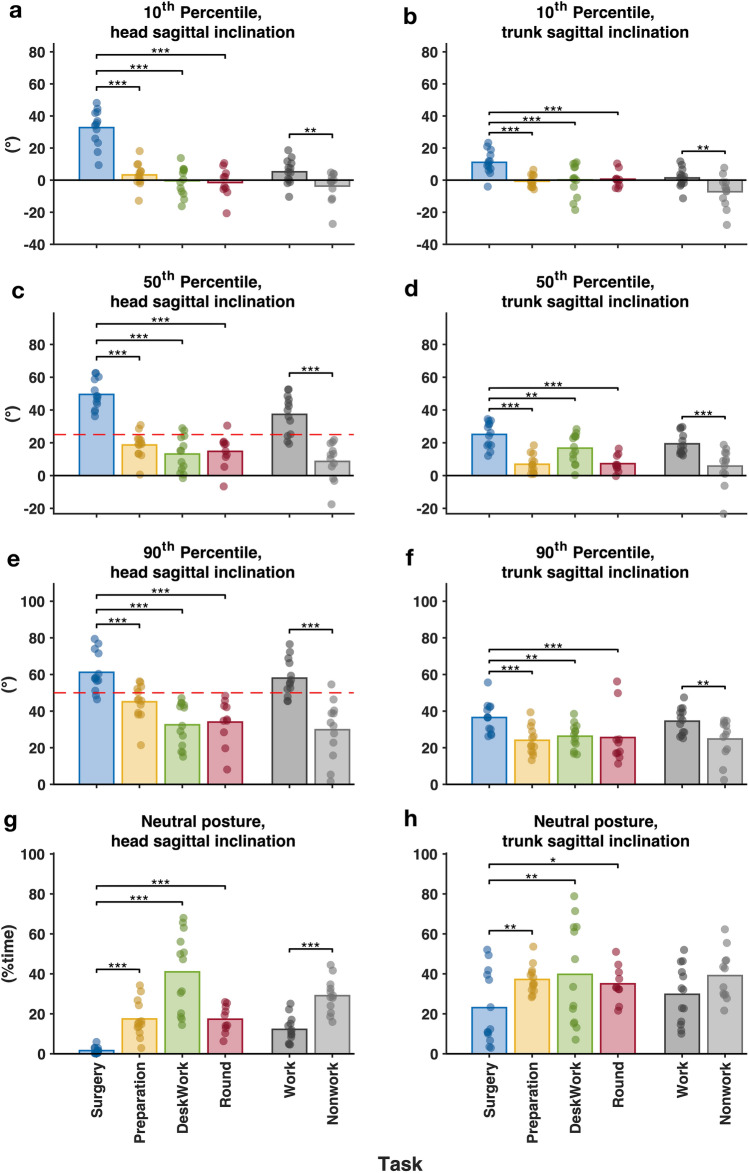
Results: Open surgery constituted more than half of a surgical workday. It was associated with more awkward postures of the head and trunk than nonsurgical tasks. It was also associated with higher trapezius muscle activity levels, less muscle rest time and a higher proportion of sustained low muscle activity than nonsurgical tasks and the two roles in RAS. The head inclination and trapezius activity in open surgery exceeded the proposed action levels.
Conclusions: The physical workload of surgeons in open surgery, which exceeded the proposed action levels, was higher than that in RAS and that in nonsurgical tasks. Demands of increased operation time may result in higher physical workload for open surgeons, which poses an increased risk of MSDs. Risk-reducing measures are, therefore, needed.
Keywords: Inclinometry; Muscle activity; Musculoskeletal disorders; Rationalization; Surgical ergonomics; Task-based analysis.
© 2022. The Author(s).
Conflict of interest statement
Xuelong Fan, Professor Mikael Forsman, Dr. Liyun Yang, Dr. Carl M. Lind, and Professor Magnus Kjellman (M.D.) have no conflicts of interest or financial ties to disclose.
Figures




Similar articles
-
Experience implication in subjective surgical ergonomics comparison between laparoscopic and robot-assisted surgeries.J Robot Surg. 2020 Feb;14(1):115-121. doi: 10.1007/s11701-019-00933-2. Epub 2019 Mar 12. J Robot Surg. 2020. PMID: 30863913
-
Intraoperative workload in robotic surgery assessed by wearable motion tracking sensors and questionnaires.Surg Endosc. 2017 Feb;31(2):877-886. doi: 10.1007/s00464-016-5047-y. Epub 2016 Aug 5. Surg Endosc. 2017. PMID: 27495330
-
Save our surgeons (SOS) - an explorative comparison of surgeons' muscular and cardiovascular demands, posture, perceived workload and discomfort during robotic vs. laparoscopic surgery.Arch Gynecol Obstet. 2023 Mar;307(3):849-862. doi: 10.1007/s00404-022-06841-5. Epub 2022 Nov 19. Arch Gynecol Obstet. 2023. PMID: 36401096 Free PMC article.
-
Ergonomics in Surgery: A Review.Female Pelvic Med Reconstr Surg. 2018 Jan/Feb;24(1):1-12. doi: 10.1097/SPV.0000000000000456. Female Pelvic Med Reconstr Surg. 2018. PMID: 28914699 Review.
-
Ergonomics in gynecologic surgery.Curr Opin Obstet Gynecol. 2018 Dec;30(6):432-440. doi: 10.1097/GCO.0000000000000502. Curr Opin Obstet Gynecol. 2018. PMID: 30299323 Review.
Cited by
-
Mental workload during endoscopic sinus surgery is associated with surgeons' skill levels.Front Med (Lausanne). 2023 Apr 24;10:1090743. doi: 10.3389/fmed.2023.1090743. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37168266 Free PMC article.
-
The role of ergonomics training and posture exercises in surgeons' musculoskeletal system disorders.Turk J Surg. 2024 Sep 30;40(3):204-211. doi: 10.47717/turkjsurg.2024.6413. eCollection 2024 Sep. Turk J Surg. 2024. PMID: 39917397 Free PMC article.
-
A New Approach to Quantifying Muscular Fatigue Using Wearable EMG Sensors during Surgery: An Ergonomic Case Study.Sensors (Basel). 2023 Feb 3;23(3):1686. doi: 10.3390/s23031686. Sensors (Basel). 2023. PMID: 36772729 Free PMC article.
-
Intraoperative workload of the surgeon in robot-assisted radical prostatectomy: a systematic review.J Robot Surg. 2024 Jul 22;18(1):289. doi: 10.1007/s11701-024-02049-8. J Robot Surg. 2024. PMID: 39039389
-
Wearable Motion Capture Devices for the Prevention of Work-Related Musculoskeletal Disorders in Ergonomics-An Overview of Current Applications, Challenges, and Future Opportunities.Sensors (Basel). 2023 Apr 25;23(9):4259. doi: 10.3390/s23094259. Sensors (Basel). 2023. PMID: 37177463 Free PMC article. Review.
References
-
- Lloyd GL, Chung ASJ, Steinberg S, Sawyer M, Williams DH, Overbey D. Is your career hurting you? The ergonomic consequences of surgery in 701 urologists worldwide. J Endourol. 2019;33:1037–1042. - PubMed
-
- Howarth AL, Hallbeck S, Mahabir RC, Lemaine V, GregoryR D, Evans NSS. Work-related musculoskeletal discomfort and injury in microsurgeons. J Reconstr Microsurg. 2019;35:322–328. - PubMed
-
- Howarth AL, Hallbeck MS, Lemaine V, Singh DJ, Noland SS. Work-related musculoskeletal discomfort and injury in craniofacial and maxillofacial surgeons. J Craniofac Surg. 2019;30:1982–1985. - PubMed
-
- Lobo D, Gandarillas MA, Sánchez-Gómez S, Megía R. Work-related musculoskeletal symptoms in otorhinolaryngology and their relationship with physical activity A Nationwide Survey. J Laryngol Otol. 2019;133:713–718. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
