

Inertial Sensor-to-Segment Calibration for Accurate 3D Joint Angle Calculation for Use in OpenSim
- PMID: 35590949
- PMCID: PMC9104520
- DOI: 10.3390/s22093259
Inertial Sensor-to-Segment Calibration for Accurate 3D Joint Angle Calculation for Use in OpenSim
Abstract
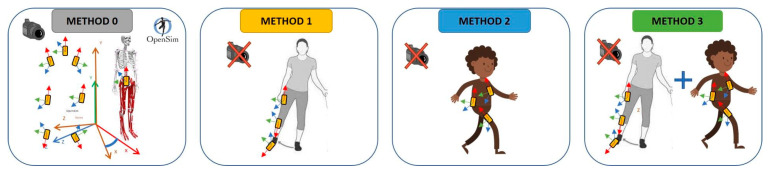
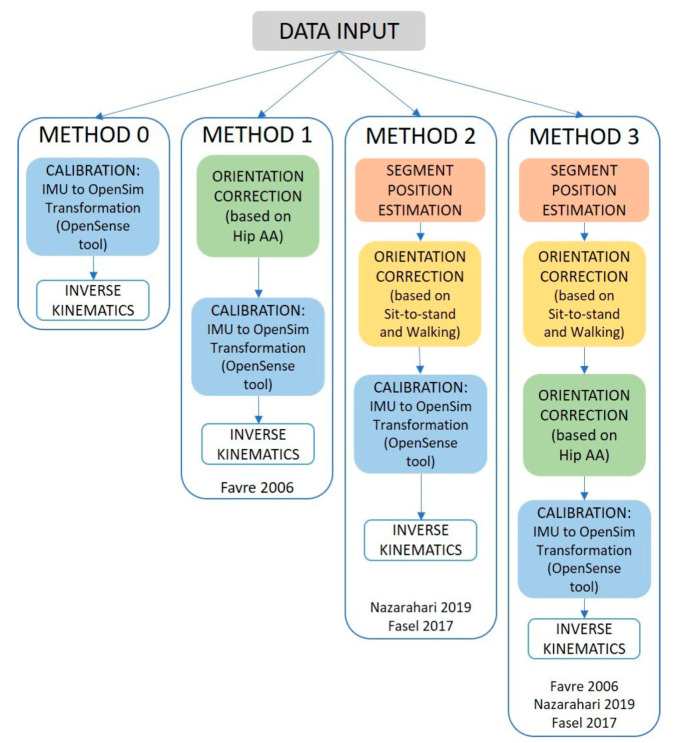
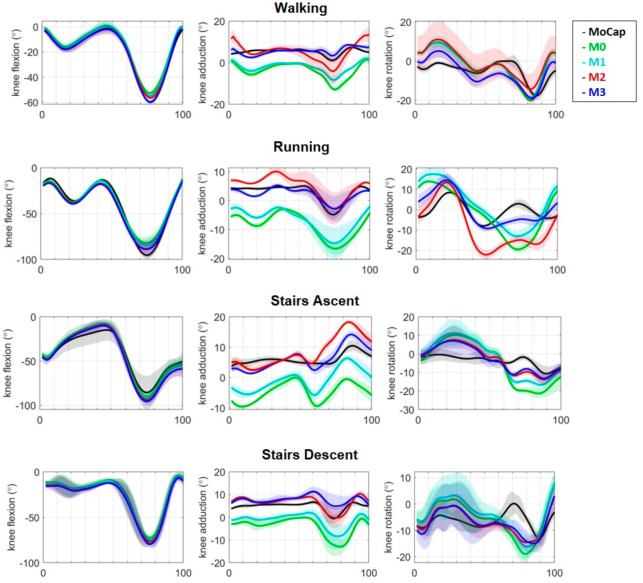
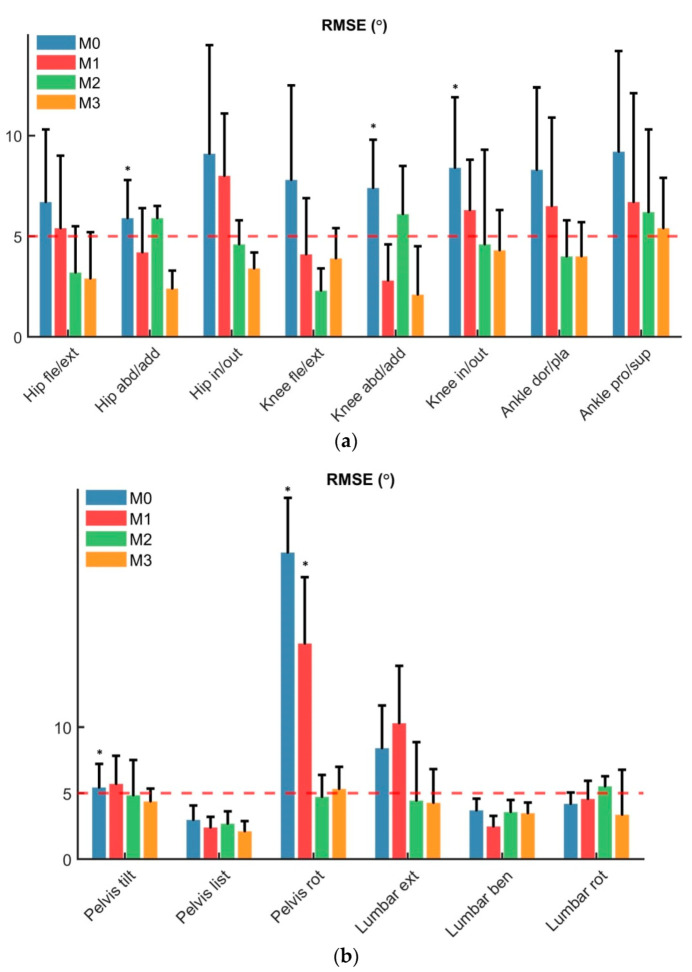
Inertial capture (InCap) systems combined with musculoskeletal (MSK) models are an attractive option for monitoring 3D joint kinematics in an ecological context. However, the primary limiting factor is the sensor-to-segment calibration, which is crucial to estimate the body segment orientations. Walking, running, and stair ascent and descent trials were measured in eleven healthy subjects with the Xsens InCap system and the Vicon 3D motion capture (MoCap) system at a self-selected speed. A novel integrated method that combines previous sensor-to-segment calibration approaches was developed for use in a MSK model with three degree of freedom (DOF) hip and knee joints. The following were compared: RMSE, range of motion (ROM), peaks, and R2 between InCap kinematics estimated with different calibration methods and gold standard MoCap kinematics. The integrated method reduced the RSME for both the hip and the knee joints below 5°, and no statistically significant differences were found between MoCap and InCap kinematics. This was consistent across all the different analyzed movements. The developed method was integrated on an MSK model workflow, and it increased the sensor-to-segment calibration accuracy for an accurate estimate of 3D joint kinematics compared to MoCap, guaranteeing a clinical easy-to-use approach.
Keywords: 3D joint kinematics; IMU; biomechanical model; joint angles; lower-body kinematics; motion analysis; musculoskeletal; open-source; sensor-to-segment calibration; wearable sensors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Estimation of 3D Knee Joint Angles during Cycling Using Inertial Sensors: Accuracy of a Novel Sensor-to-Segment Calibration Procedure Based on Pedaling Motion.Sensors (Basel). 2019 May 30;19(11):2474. doi: 10.3390/s19112474. Sensors (Basel). 2019. PMID: 31151200 Free PMC article. Clinical Trial.
-
Sagittal plane knee kinematics can be measured during activities of daily living following total knee arthroplasty with two IMU.PLoS One. 2024 Feb 15;19(2):e0297899. doi: 10.1371/journal.pone.0297899. eCollection 2024. PLoS One. 2024. PMID: 38359050 Free PMC article.
-
Validation of wearable inertial sensor-based gait analysis system for measurement of spatiotemporal parameters and lower extremity joint kinematics in sagittal plane.Proc Inst Mech Eng H. 2022 May;236(5):686-696. doi: 10.1177/09544119211072971. Epub 2022 Jan 8. Proc Inst Mech Eng H. 2022. PMID: 35001713
-
Monitoring Methods of Human Body Joints: State-of-the-Art and Research Challenges.Sensors (Basel). 2019 Jun 10;19(11):2629. doi: 10.3390/s19112629. Sensors (Basel). 2019. PMID: 31185629 Free PMC article. Review.
-
Methods for Gastrointestinal Endoscopy Quantification: A Focus on Hands and Fingers Kinematics.Sensors (Basel). 2022 Nov 28;22(23):9253. doi: 10.3390/s22239253. Sensors (Basel). 2022. PMID: 36501954 Free PMC article. Review.
Cited by
-
Gait Alteration in Individual with Limb Loss: The Role of Inertial Sensors.Sensors (Basel). 2023 Feb 7;23(4):1880. doi: 10.3390/s23041880. Sensors (Basel). 2023. PMID: 36850475 Free PMC article. Review.
-
Quantification of 3D Kinematic Measurements for Knee Flexion and Tibial Rotation Using an IMU-Based Sensor and Ultrasound Imaging System: A Cadaveric Study.Sensors (Basel). 2025 Jul 6;25(13):4211. doi: 10.3390/s25134211. Sensors (Basel). 2025. PMID: 40648466 Free PMC article.
-
SensAA-Design and Verification of a Cloud-Based Wearable Biomechanical Data Acquisition System.Sensors (Basel). 2024 Apr 9;24(8):2405. doi: 10.3390/s24082405. Sensors (Basel). 2024. PMID: 38676022 Free PMC article.
-
Machine Learning for Optical Motion Capture-Driven Musculoskeletal Modelling from Inertial Motion Capture Data.Bioengineering (Basel). 2023 Apr 24;10(5):510. doi: 10.3390/bioengineering10050510. Bioengineering (Basel). 2023. PMID: 37237580 Free PMC article.
-
The Automatization of the Gait Analysis by the Vicon Video System: A Pilot Study.Sensors (Basel). 2022 Sep 21;22(19):7178. doi: 10.3390/s22197178. Sensors (Basel). 2022. PMID: 36236276 Free PMC article.
References
-
- Karatsidis A., Richards R.E., Konrath J.M., van den Noort J.C., Schepers H.M., Bellusci G., Harlaar J., Veltink P.H. Validation of wearable visual feedback for retraining foot progression angle using inertial sensors and an augmented reality headset. J. Neuroeng. Rehabil. 2018;15:78. doi: 10.1186/s12984-018-0419-2. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
