

Intra- and Inter-Subject Perspectives on the Detection of Focal Onset Motor Seizures in Epilepsy Patients
- PMID: 35591007
- PMCID: PMC9105312
- DOI: 10.3390/s22093318
Intra- and Inter-Subject Perspectives on the Detection of Focal Onset Motor Seizures in Epilepsy Patients
Abstract
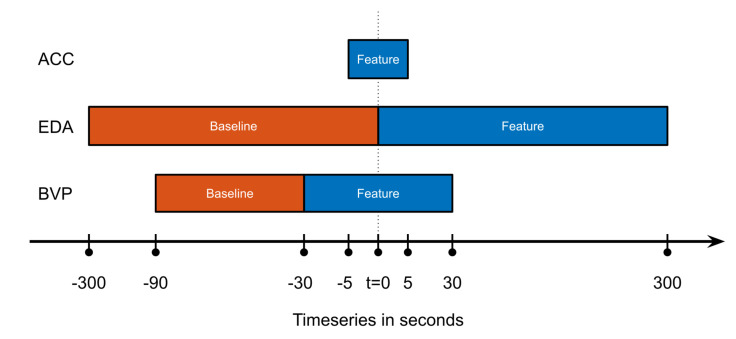
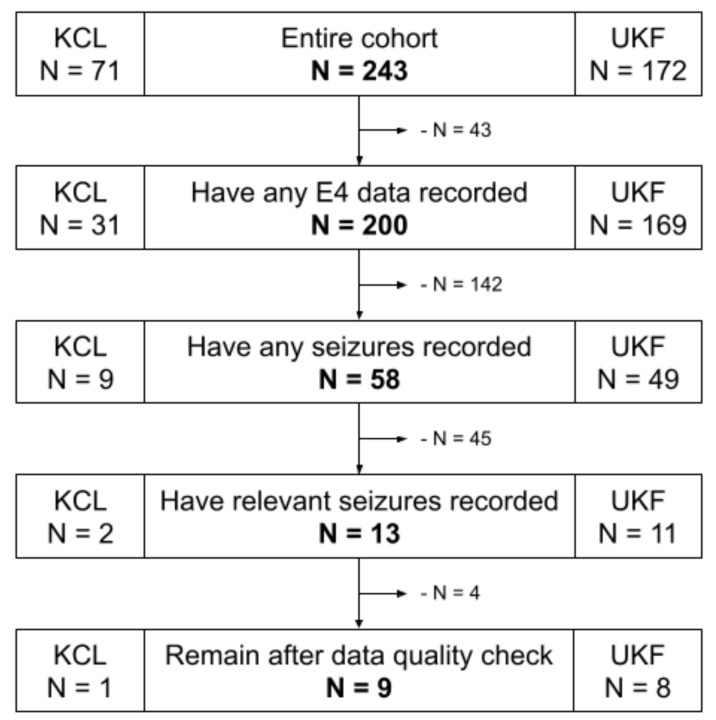
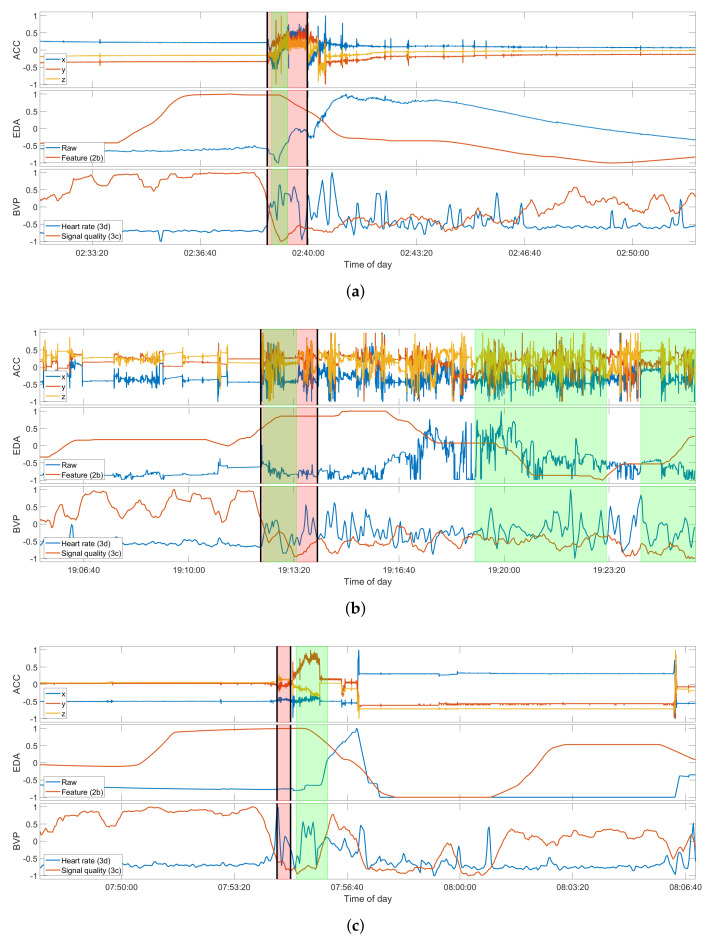
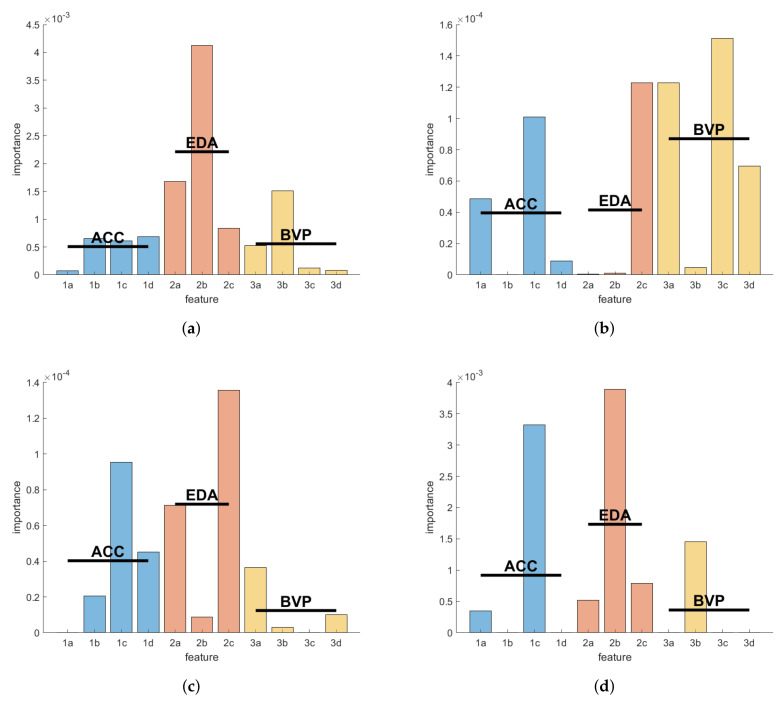
Focal onset epileptic seizures are highly heterogeneous in their clinical manifestations, and a robust seizure detection across patient cohorts has to date not been achieved. Here, we assess and discuss the potential of supervised machine learning models for the detection of focal onset motor seizures by means of a wrist-worn wearable device, both in a personalized context as well as across patients. Wearable data were recorded in-hospital from patients with epilepsy at two epilepsy centers. Accelerometry, electrodermal activity, and blood volume pulse data were processed and features for each of the biosignal modalities were calculated. Following a leave-one-out approach, a gradient tree boosting machine learning model was optimized and tested in an intra-subject and inter-subject evaluation. In total, 20 seizures from 9 patients were included and we report sensitivities of 67% to 100% and false alarm rates of down to 0.85 per 24 h in the individualized assessment. Conversely, for an inter-subject seizure detection methodology tested on an out-of-sample data set, an optimized model could only achieve a sensitivity of 75% at a false alarm rate of 13.4 per 24 h. We demonstrate that robustly detecting focal onset motor seizures with tonic or clonic movements from wearable data may be possible for individuals, depending on specific seizure manifestations.
Keywords: digital health; eHealth; epilepsy; mHealth; mobile health; multimodal; seizure detection; wearables.
Conflict of interest statement
A.S. receives research funding from the German Ministry of Science, European Union, National Institute of Health, and from the companies BIAL, Precisis, and UNEEG; is an advisory board member of SEER Medical; and has received honoraria for lectures or advice from Arvelle, BIAL, EISAI, GW, Precisis, and UCB. M.P.R. holds or co-holds research funding from the UK Medical Research Council, UK National Institute for Health Research, Wellcome Trust, UK Engineering and Physical Sciences Research Council, Epilepsy Research UK, Epilepsy Foundation of America, European Commission, Canadian Institutes of Health Research, Xenon Pharma, and GW Pharma; has research collaborations with UNEEG Medical, Seer Medical, UCB Pharma, ANT Neuro, and IMEC; is a Trustee of Epilepsy Research UK and an advisory board member of SUDEP Action; M.P.R. does not receive personal remuneration from any of these sources. M.P.R. holds a patent WO2013182848A1. V.T. is an employee of UCB Pharma.
Figures

References
-
- Fisher R.S., Cross J.H., French J.A., Higurashi N., Hirsch E., Jansen F.E., Lagae L., Moshé S.L., Peltola J., Roulet Perez E., et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017;58:522–530. doi: 10.1111/epi.13670. - DOI - PubMed
-
- Schulze-Bonhage A., Bruno E., Brandt A., Shek A., Heers M., Martinez-Lizana E., Altenmüller D.M., Richardson M.P., San Antonio V. Diagnostic yield and limitations of in-hospital documentation in patients with epilepsy. Epilepsia. 2022 in press . - PubMed
-
- Beniczky S., Wiebe S., Jeppesen J., Tatum W.O., Brazdil M., Wang Y., Herman S.T., Ryvlin P. Automated seizure detection using wearable devices: A clinical practice guideline of the International League Against Epilepsy and the International Federation of Clinical Neurophysiology. Epilepsia. 2021;62:632–646. doi: 10.1111/epi.16818. - DOI - PubMed
-
- Brinkmann B.H., Karoly P.J., Nurse E.S., Dumanis S.B., Nasseri M., Viana P.F., Schulze-Bonhage A., Freestone D.R., Worrell G., Richardson M.P., et al. Seizure Diaries and Forecasting With Wearables: Epilepsy Monitoring Outside the Clinic. Front. Neurol. 2021;12:1–14. doi: 10.3389/fneur.2021.690404. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
