

The use of technology-based adherence monitoring in the treatment of hepatitis C virus
- PMID: 35591885
- PMCID: PMC9112320
- DOI: 10.1177/20499361221095664
The use of technology-based adherence monitoring in the treatment of hepatitis C virus
Abstract
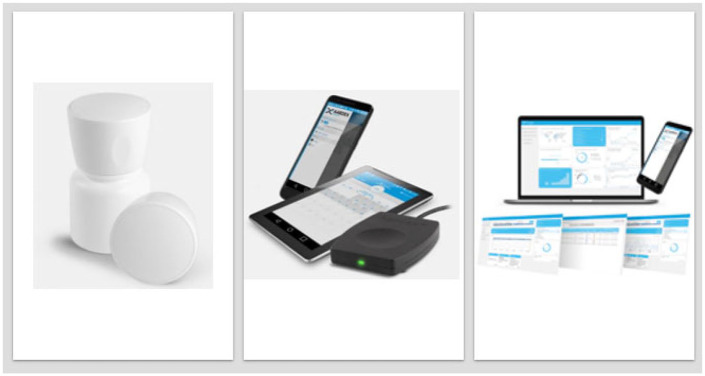
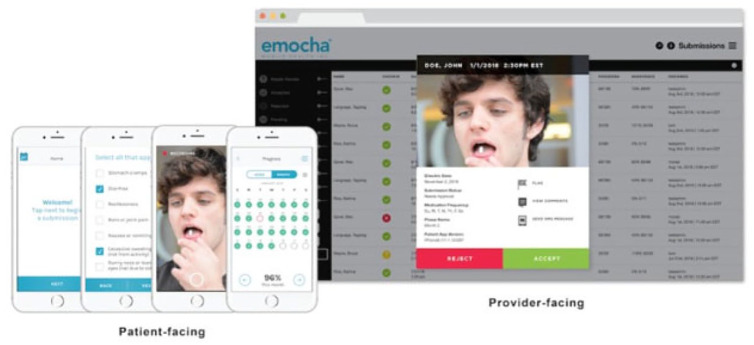
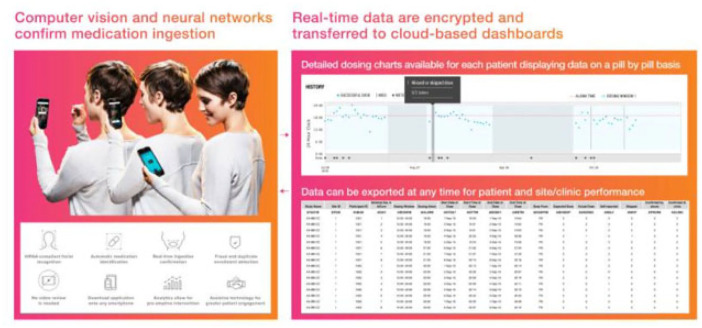
Direct-acting antivirals (DAAs) achieve high hepatitis C virus (HCV) cure rates and are forgiving to missed doses, but adherence-efficacy relationships have not been well defined. Traditional adherence measures (e.g. pill counts, self-report and pharmacy refills) over-estimate medication adherence. Newer technology-based tools have been used to provide more objective adherence data. Herein, electronic medication diaries (e-diaries), medication events monitoring system (MEMS®) caps, electronic blister packs, electronic pill boxes, video-based directly observed therapy (vDOT), artificial intelligence platforms (AIPs), and ingestible sensor systems are described, and compared based on existing studies using DAA. Percent adherence, predictors of adherence, and HCV cure rates utilizing these technologies are included. DAA adherence with e-diaries was 95-96%, MEMS® caps and ingestible biosensors were between 95% and 97%, blister pack weekly dosing ranged 73-98%, and daily dosing 73-94%, whereas electronic pill boxes ranged between 39% and 89%, vDOT was 98% and AIP 91-96%. Despite a wide range of adherence, high sustained virologic response (SVR) rates (86-100%) were observed across all studies utilizing these different technology-based tools. Current data support the forgiveness of DAA therapies to missed doses using tools that provide more quantitative adherence measures compared with self-report and provide insight on adherence-efficacy relationships for contemporary DAA.
Keywords: DAA; SVR; adherence; hepatitis C; technology-based tools.
© The Author(s), 2022.
Conflict of interest statement
Conflict of interest statement: The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PLA has received consulting fees from Merck and ViiV. The remaining authors declared no conflicts of interest.
Figures




References
-
- Bartenschlager R, Sparacio S. Hepatitis C virus molecular clones and their replication capacity in vivo and in cell culture. Virus Res 2007; 127: 195–207. - PubMed
-
- World Health Organization. Hepatitis C, https://www.who.int/news-room/fact-sheets/detail/hepatitis-c
-
- Deutsch M, Hadziyannis SJ. Old and emerging therapies in chronic hepatitis C: an update. J Viral Hepat 2008; 15: 2–11. - PubMed
-
- Cunningham EB, Amin J, Feld JJ, et al. Adherence to sofosbuvir and velpatasvir among people with chronic HCV infection and recent injection drug use: the SIMPLIFY study. Int J Drug Policy 2018; 62: 14–23. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
