

Prognostic Impact of Multiple Lymphocyte-Based Inflammatory Indices in Acute Coronary Syndrome Patients
- PMID: 35592392
- PMCID: PMC9110784
- DOI: 10.3389/fcvm.2022.811790
Prognostic Impact of Multiple Lymphocyte-Based Inflammatory Indices in Acute Coronary Syndrome Patients
Abstract
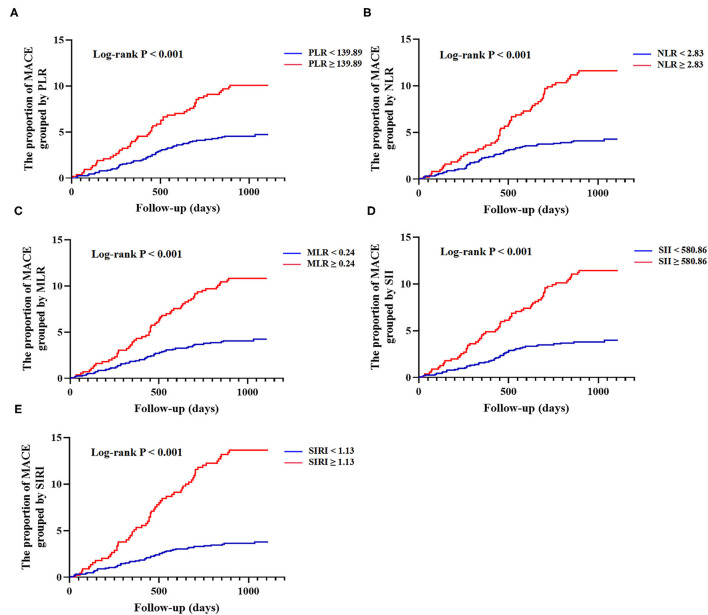
Background: The aim of this study was to evaluate the prognostic values of five lymphocyte-based inflammatory indices (platelet-lymphocyte ratio [PLR], neutrophil-lymphocyte ratio [NLR], monocyte-lymphocyte ratio [MLR], systemic immune inflammation index [SII], and system inflammation response index [SIRI]) in patients with acute coronary syndrome (ACS).
Methods: A total of 1,701 ACS patients who underwent percutaneous coronary intervention (PCI) were included in this study and followed up for major adverse cardiovascular events (MACE) including all-cause death, non-fatal ischemic stroke, and non-fatal myocardial infarction. The five indices were stratified by the optimal cutoff value for comparison. The association between each of the lymphocyte-based inflammatory indices and MACE was assessed by the Cox proportional hazards regression analysis.
Results: During the median follow-up of 30 months, 107 (6.3%) MACE were identified. The multivariate COX analysis showed that all five indices were independent predictors of MACE, and SIRI seemingly performed best (Hazard ratio [HR]: 3.847; 95% confidence interval [CI]: [2.623-5.641]; p < 0.001; C-statistic: 0.794 [0.731-0.856]). The addition of NLR, MLR, SII, or SIRI to the Global Registry of Acute Coronary Events (GRACE) risk score, especially SIRI (C-statistic: 0.699 [0.646-0.753], p < 0.001; net reclassification improvement [NRI]: 0.311 [0.209-0.407], p < 0.001; integrated discrimination improvement [IDI]: 0.024 [0.010-0.046], p < 0.001), outperformed the GRACE risk score alone in the risk predictive performance.
Conclusion: Lymphocyte-based inflammatory indices were significantly and independently associated with MACE in ACS patients who underwent PCI. SIRI seemed to be better than the other four indices in predicting MACE, and the combination of SIRI with the GRACE risk score could predict MACE more accurately.
Keywords: GRACE risk score; acute coronary syndrome; lymphocyte-based inflammatory indices; major adverse cardiovascular events; percutaneous coronary intervention.
Copyright © 2022 Li, Ma, Shao, Yang, Wang, Gao, Zhou, Yang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous