

Chest wall mechanics during mechanical chest compression and its relationship to CPR-related injuries and survival
- PMID: 35592875
- PMCID: PMC9112017
- DOI: 10.1016/j.resplu.2022.100242
Chest wall mechanics during mechanical chest compression and its relationship to CPR-related injuries and survival
Abstract
Aim: To determine compression force variation (CFV) during mechanical cardiopulmonary resuscitation (CPR) and its relationship with CPR-related injuries and survival.
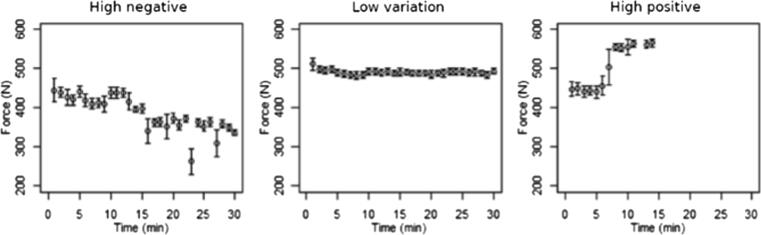
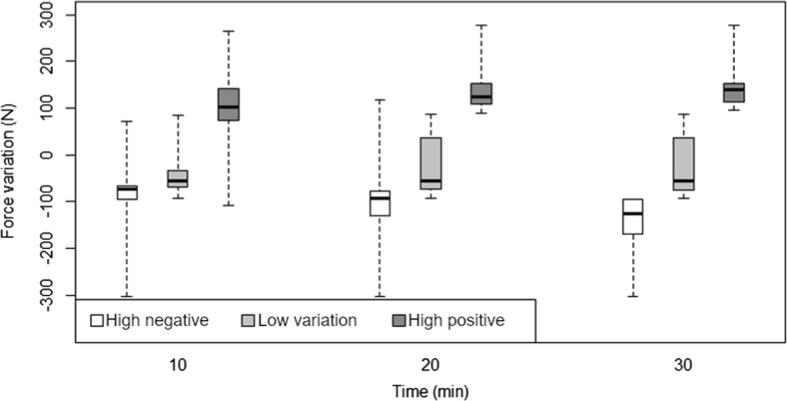
Methods: Adult non-traumatic OHCA patients who had been treated with mechanical CPR were evaluated for CPR-related injuries using chest X-rays, thoracic computed tomography or autopsy. The CFV exerted by the LUCAS 2 device was calculated as the difference between the maximum and the minimum force values and was categorised into three different groups (high positive CFV ≥ 95 newton (N), high negative CFV ≤ -95 N, and low variation for intermediate CFV). The CFV was correlated with the CPR injuries findings and survival data.
Results: Fifty-two patients were included. The median (IQR) age was 57 (49-66) years, and 13 (25%) cases survived until hospital admission. High positive CFV was found in 21 (40.4%) patients, high negative CFV in 9 (17.3%) and a low CFV in 22 (42.3%). The median (IQR) number of rib fractures was higher in the high positive and negative CFV groups compared with the low CFV group [7(1-9) and 9 (4-11) vs 0 (0-6) (p = 0.021)]. More bilateral fracture cases were found in the high positive and negative CFV groups [16 (76.2%) and 6 (66.7%) vs 6 (27.3%) (p = 0.004)]. In the younger half of the sample more patients survived until hospital admission in the low CFV group compared with the high CFV groups [5 (41.7%) vs 1 (7.1%) (p = 0.037)].
Conclusions: High CFV was associated with ribcage injuries. In the younger patients low CFV was associated with survival until hospital admission.
Keywords: Cardiopulmonary resuscitation; Out-of-hospital cardiac arrest; Sudden death; Thoracic injuries.
© 2022 The Author(s).
Figures
References
-
- Handley A.J. Press hard – But perhaps not too hard. Resuscitation. 2014;85:153–154. - PubMed
-
- Cone D.C. Push hard, push fast, do not stop—optimal chest compression rate and depth. JAMA Cardiol. 2019;4:908. - PubMed
-
- Karasek J., Slezak J., Stefela R., Topinka M., Blankova A., Doubková A., et al. CPR-related injuries after non-traumatic out-of-hospital cardiac arrest: survivors versus non-survivors. Resuscitation. 2022;171:90–95. - PubMed
-
- Azeli Y., Barbería E., Jiménez-Herrera M., Ameijide A., Axelsson C., Bardají A. Serious injuries secondary to cardiopulmonary resuscitation: incidence and associated factors. Emergencias. 2019;31:327–334. - PubMed
LinkOut - more resources
Full Text Sources
