

Plasma MIA, CRP, and Albumin Predict Cognitive Decline in Parkinson's Disease
- PMID: 35593028
- PMCID: PMC9329215
- DOI: 10.1002/ana.26410
Plasma MIA, CRP, and Albumin Predict Cognitive Decline in Parkinson's Disease
Abstract
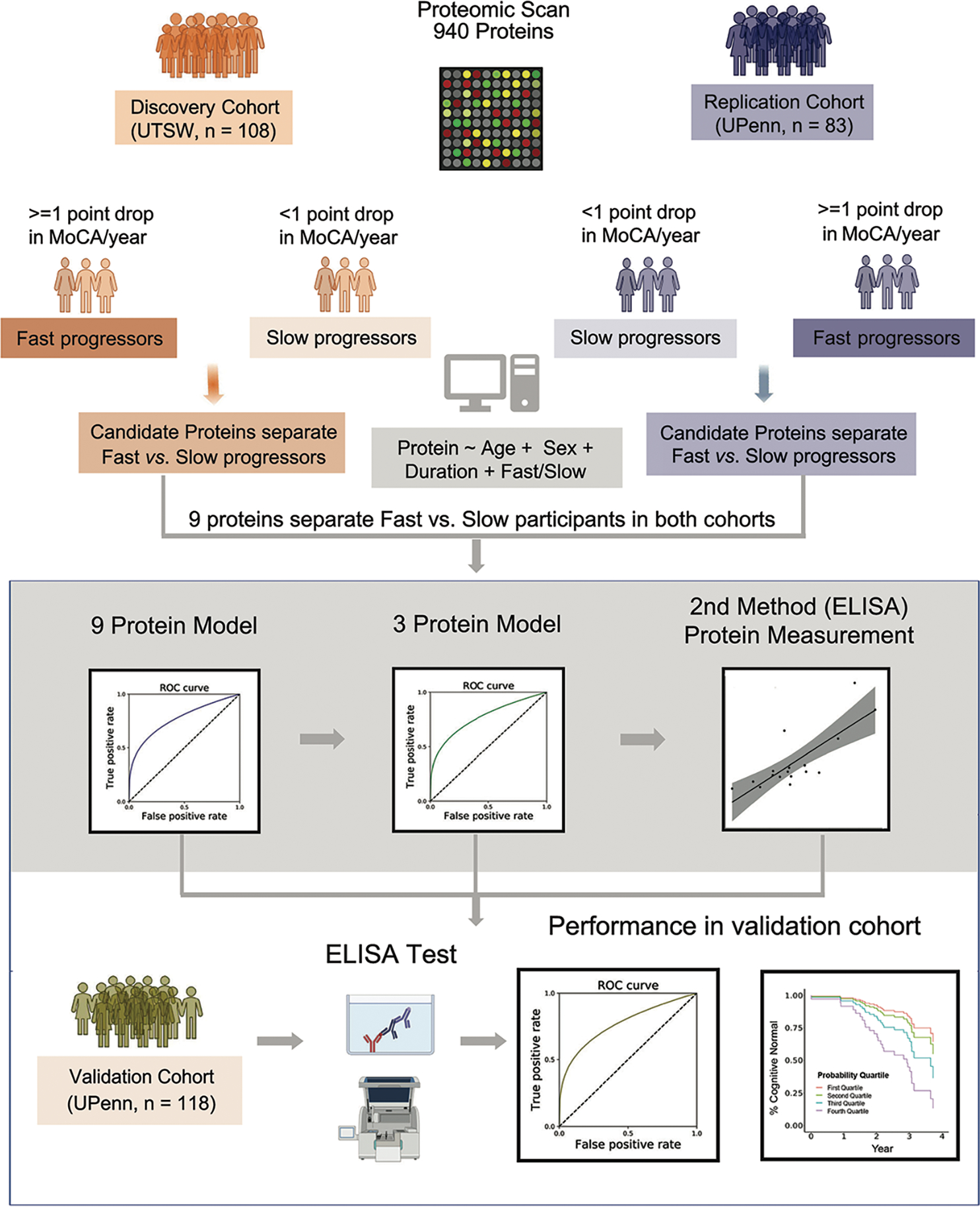
Objective: Using a multi-cohort, discovery-replication-validation design, we sought new plasma biomarkers that predict which individuals with Parkinson's disease (PD) will experience cognitive decline.
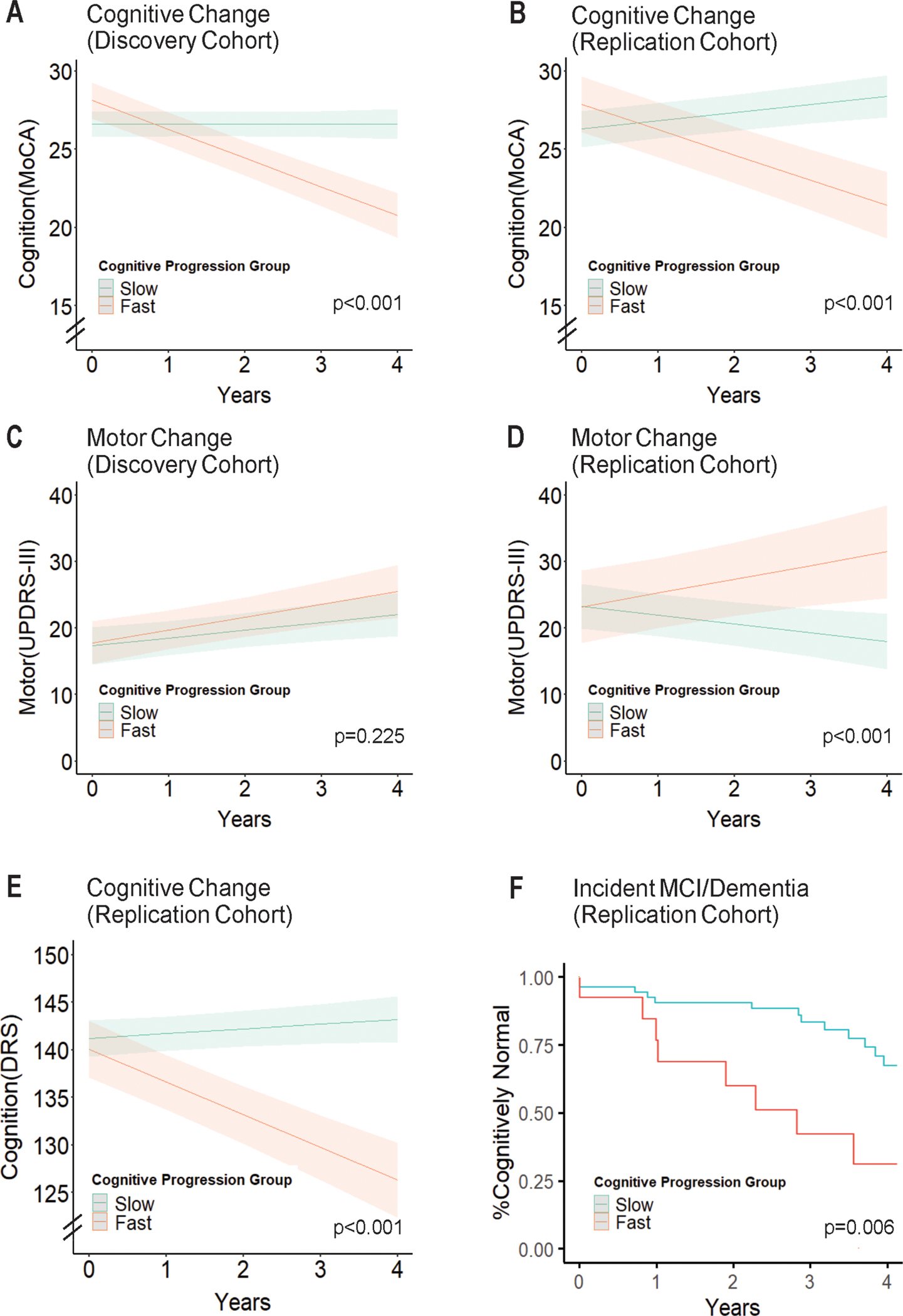
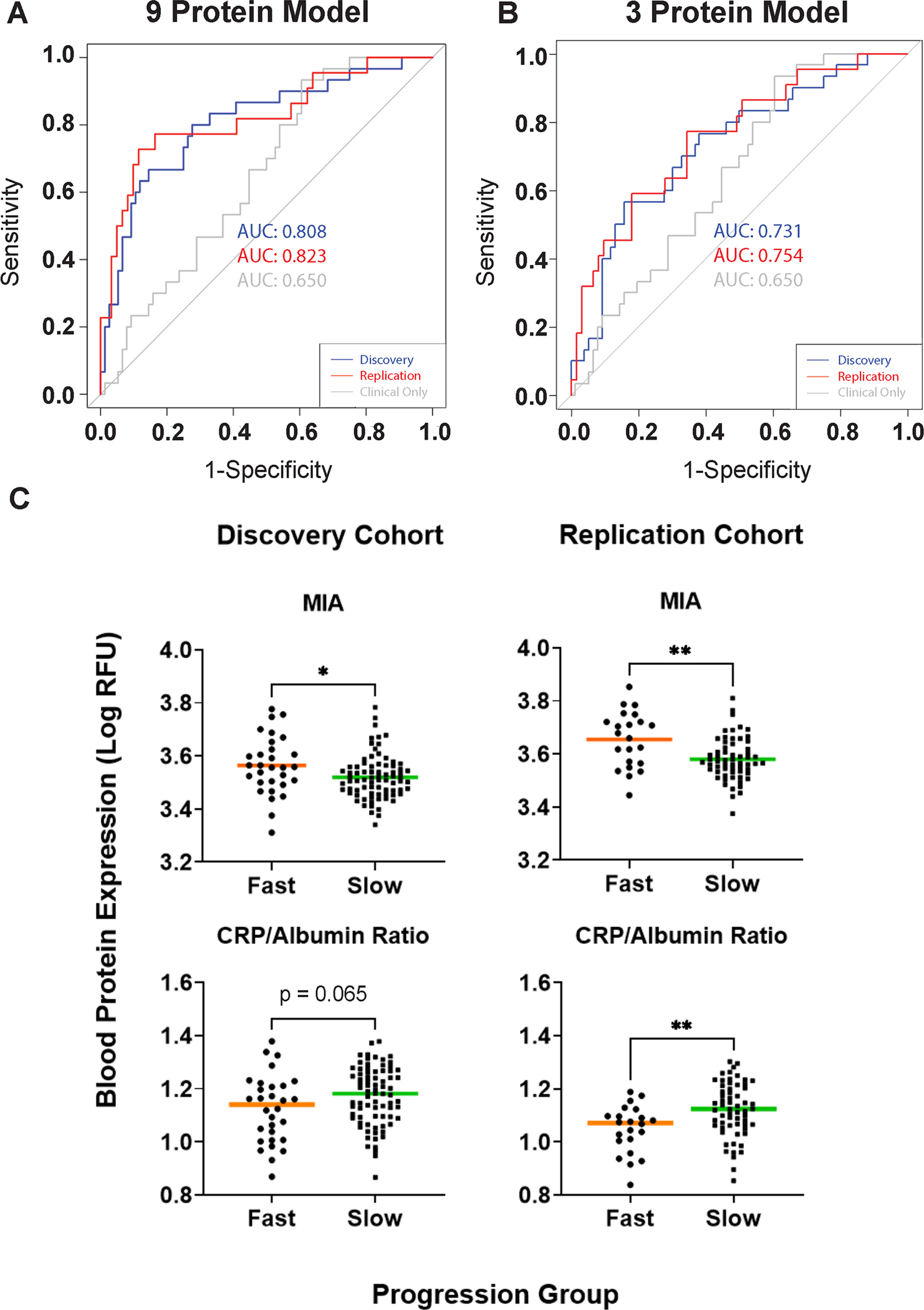
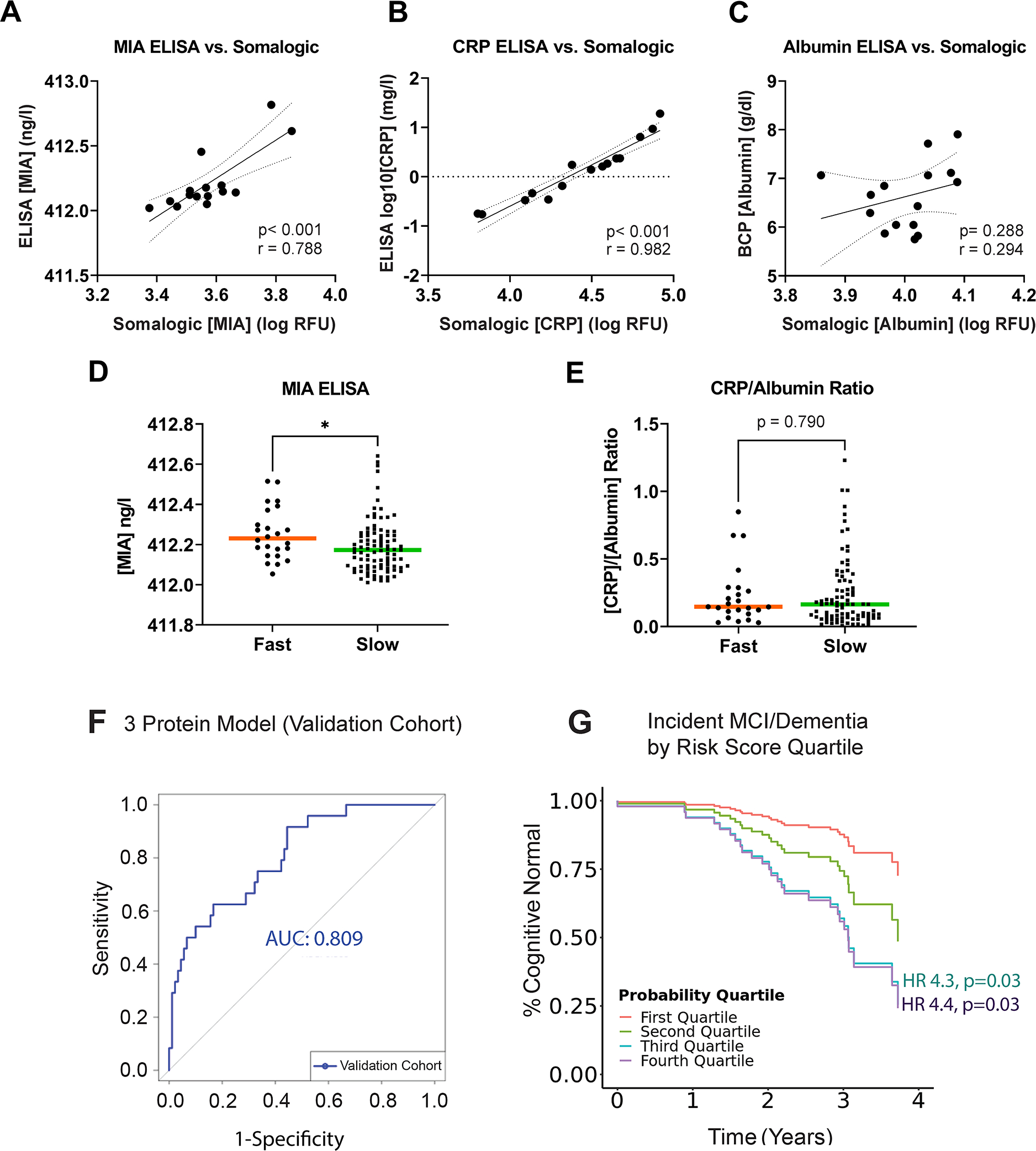
Methods: In 108 discovery cohort PD individuals and 83 replication cohort PD individuals, we measured 940 plasma proteins on an aptamer-based platform. Using proteins associated with subsequent cognitive decline in both cohorts, we trained a logistic regression model to predict which patients with PD showed fast (> = 1 point drop/year on Montreal Cognitive Assessment [MoCA]) versus slow (< 1 point drop/year on MoCA) cognitive decline in the discovery cohort, testing it in the replication cohort. We developed alternate assays for the top 3 proteins and confirmed their ability to predict cognitive decline - defined by change in MoCA or development of incident mild cognitive impairment (MCI) or dementia - in a validation cohort of 118 individuals with PD. We investigated the top plasma biomarker for causal influence by Mendelian randomization (MR).
Results: A model with only 3 proteins (melanoma inhibitory activity protein [MIA], C-reactive protein [CRP], and albumin) separated fast versus slow cognitive decline subgroups with an area under the curve (AUC) of 0.80 in the validation cohort. The individuals with PD in the validation cohort in the top quartile of risk for cognitive decline based on this model were 4.4 times more likely to develop incident MCI or dementia than those in the lowest quartile. Genotypes at MIA single nucleotide polymorphism (SNP) rs2233154 associated with MIA levels and cognitive decline, providing evidence for MIA's causal influence.
Conclusions: An easily obtained plasma-based predictor identifies individuals with PD at risk for cognitive decline. MIA may participate causally in development of cognitive decline. ANN NEUROL 2022;92:255-269.
© 2022 American Neurological Association.
Conflict of interest statement
POTENTIAL CONFLICTS OF INTEREST
Nothing to report.
Figures

References
-
- Hoehn MM, Yahr MD. Parkinsonism - Onset Progression and Mortality. Neurology. 1967;17(5):427–&. - PubMed
-
- Hely MA, Reid WGJ, Adena MA, et al. The Sydney multicenter study of Parkinson’s disease: The inevitability of dementia at 20 years. Movement Disord. 2008. Apr 30;23(6):837–44. - PubMed
-
- Aarsland D, Larsen JP, Karlsen K, et al. Mental symptoms in Parkinson’s disease are important contributors to caregiver distress. Int J Geriatr Psych. 1999. Oct;14(10):866–74. - PubMed
-
- Pressley JC, Louis ED, Tang MX, et al. The impact of comorbid disease and injuries on resource use and expenditures in parkinsonism. Neurology. 2003. Jan 14;60(1):87–93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
