

Relationship of diabetes, heart failure, and N-terminal pro-B-type natriuretic peptide with cardiovascular outcomes in patients with atrial fibrillation
- PMID: 35593128
- PMCID: PMC9288777
- DOI: 10.1002/ehf2.13930
Relationship of diabetes, heart failure, and N-terminal pro-B-type natriuretic peptide with cardiovascular outcomes in patients with atrial fibrillation
Abstract
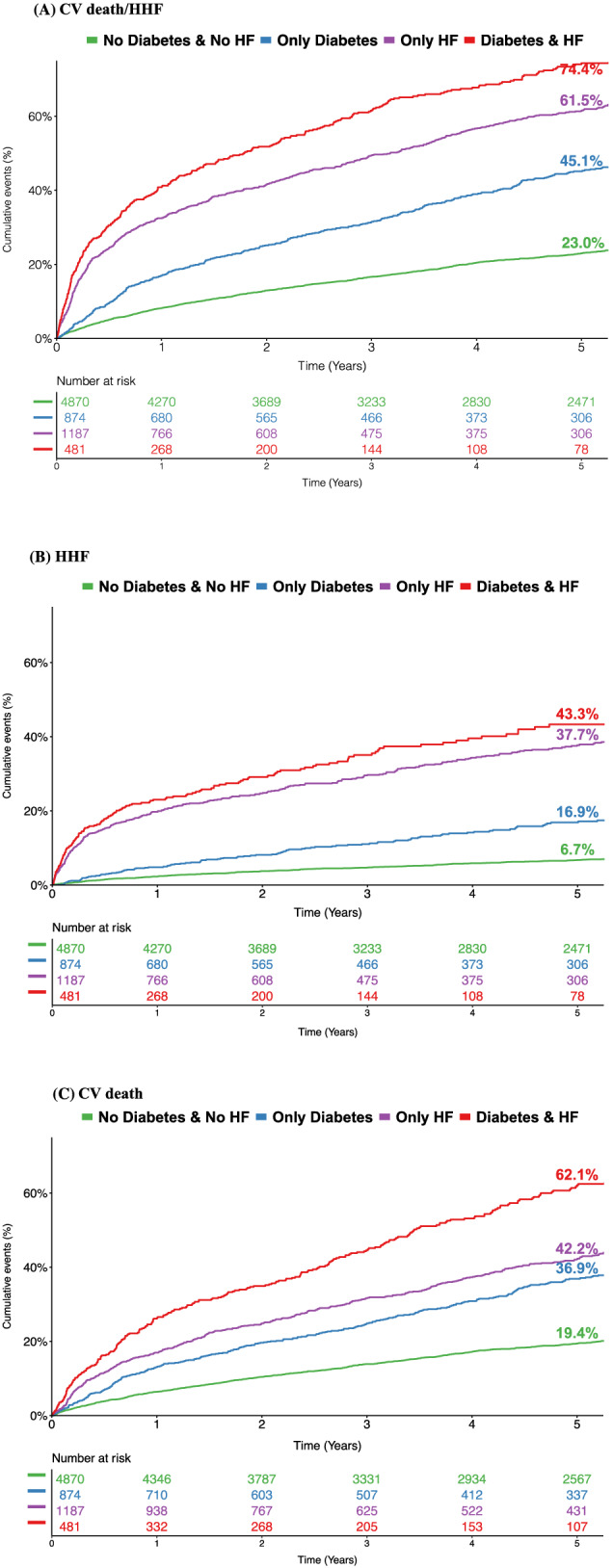
Aims: We aim to explore the relationship of heart failure (HF) and diabetes with cardiovascular (CV) death or hospitalization for HF (HHF) and to study the clinical utility of N-terminal pro-B-type natriuretic peptide (NT-proBNP) in an unselected patient population with atrial fibrillation (AF).
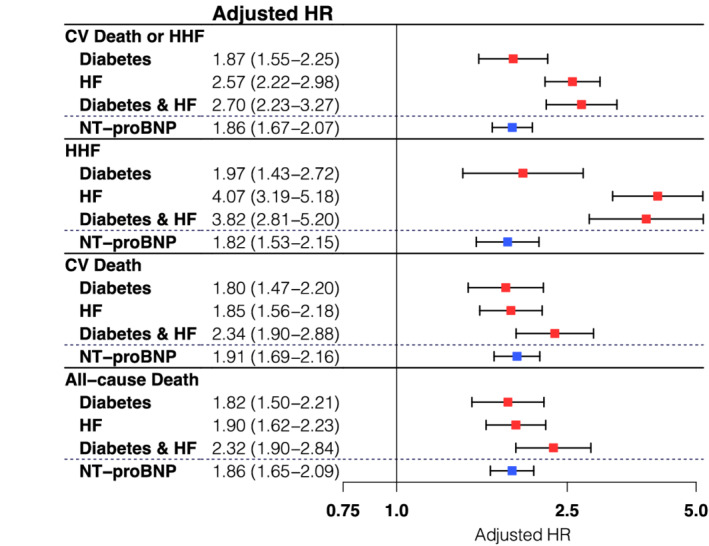
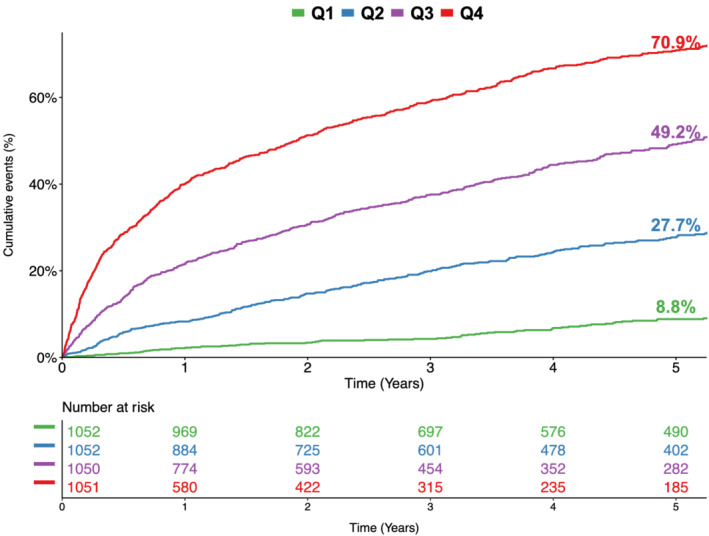
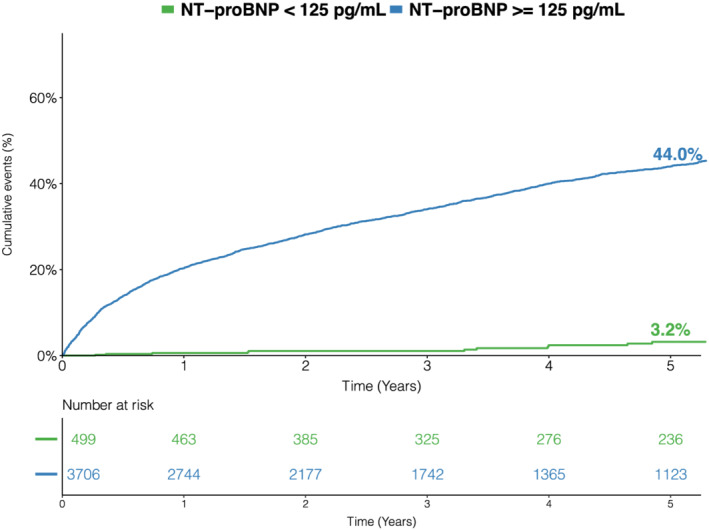
Methods and results: Patients with AF admitted to a tertiary academic center between January 2005 and July 2019 were identified through a search of electronic health records. We used Cox regression models adjusted for age, sex, estimated glomerular filtration rate, diabetes, HF, body mass index, prior myocardial infarction, coronary artery disease, hypertension, smoking, C-reactive protein, and low-density lipoprotein cholesterol. To select the most informative variables, we performed a least absolute shrinkage and selection operator Cox regression with 10-fold cross-validation. In total, 7412 patients (median age 70 years, 39.7% female) were included in this analysis and followed over a median of 4.5 years. Both diabetes [adjusted (Adj.) HR 1.87, 95% CI 1.55-2.25] and HF (Adj. HR 2.57, 95% CI 2.22-2.98) were significantly associated with CV death/HHF after multivariable adjustment. Compared with patients with diabetes, HF patients had a higher risk of HHF but a similar risk of CV and all-cause death. NT-proBNP showed good discriminatory performance (area under the curve 0.78, 95% CI 0.77-0.80) and the addition of NT-proBNP to the covariates used for adjustment resulted in a significant area under the curve improvement (Δ = 0.04, P < 0.001). With least absolute shrinkage and selection operator, the strongest associations for CV death/HHF were obtained for NT-proBNP [HR 1.91 per 1-SD in log-transformed biomarker], HF (HR 1.72), and diabetes (HR 1.56).
Conclusions: Diabetes and HF were independently associated with an increased risk of CV death/HHF in an unselected AF patient population, and NT-proBNP improved risk assessment. These findings suggest that AF patients with diabetes and/or HF should be managed not only for their risk of stroke and systemic embolic events but also for CV death/HHF.
Keywords: Atrial fibrillation; Diabetes mellitus; Heart failure; NT-proBNP.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Dr. Hofer has no conflict of interest. Dipl. Ing. Pailer has no conflict of interest. Dr. Sulzgruber reports grants from Daiichi Sankyo, grants from AstraZeneca and grants from Boehringer‐Ingelheim outside the submitted work. Dr. Gerges has received compensation for scientific symposia from Actelion, AOPOrphan Pharmaceuticals, AstraZeneca, and GlaxoSmithKline. Dr. Winter has no conflict of interest. Dr. Giugliano reports grant support from Anthos. Amgen, and Daiichi Sankyo to his institution, and honoraria for CME lectures and/or consulting from Amgen, Boeheringer‐Ingelheim, Bristol Myers Squibb, CryoLife, Daiichi Sankyo, Janssen, Pfizer, SAJA, Servier, and St Lukes Hospital System of Kansas City. Dr. Gottsauner‐Wolf reports no conflicts of interest for this study. Dr. Hülsmann reports consultant, speaker, and research support by Roche Diagnostics, consultant and speaker fee, by Boehringer, Astra Zeneca, Vifor, Novartis, Pfizer, Merck and Bayer. Dr. Kazem reports no conflict of interest. Dr. Koller reports no conflict of interest. Dr. Schönbauer reports no conflict of interest. Dr. Niessner reports personal fees from Bayer, personal fees from BMS, grants and personal fees from Boehringer Ingelheim, grants and personal fees from Daiichi Sankyo and personal fees from Pfizer outside the submitted work. Dr. Hengstenberg reports no conflicts of interest for this study. Dr. Zelniker reports research grants from the Austrian Science Funds and the German Research Foundation, honoraria for serving on advisory boards from Boehringer Ingelheim, personal fees from AstraZeneca, Boehringer Ingelheim, and Sun Pharmaceutical Industries, and educational grants from Eli Lilly and Company.
Figures
Similar articles
-
Heart Failure Risk Assessment Using Biomarkers in Patients With Atrial Fibrillation: Analysis From COMBINE-AF.J Am Coll Cardiol. 2024 Oct 15;84(16):1528-1540. doi: 10.1016/j.jacc.2024.07.023. Epub 2024 Sep 2. J Am Coll Cardiol. 2024. PMID: 39230543
-
Prognostic Value of N-Terminal Pro-B-Type Natriuretic Peptide Levels in Heart Failure Patients With and Without Atrial Fibrillation.Circ Heart Fail. 2017 Oct;10(10):e004409. doi: 10.1161/CIRCHEARTFAILURE.117.004409. Circ Heart Fail. 2017. PMID: 29018174
-
N-Terminal Pro-B-Type Natriuretic Peptide Levels for Risk Prediction in Patients With Heart Failure and Preserved Ejection Fraction According to Atrial Fibrillation Status.Circ Heart Fail. 2019 Mar;12(3):e005766. doi: 10.1161/CIRCHEARTFAILURE.118.005766. Circ Heart Fail. 2019. PMID: 30871349
-
Interactions Between Atrial Fibrillation and Natriuretic Peptide in Predicting Heart Failure Hospitalization or Cardiovascular Death.J Am Heart Assoc. 2022 Feb 15;11(4):e022833. doi: 10.1161/JAHA.121.022833. Epub 2022 Feb 3. J Am Heart Assoc. 2022. PMID: 35112889 Free PMC article.
-
Relationship of atrial fibrillation and N terminal pro brain natriuretic peptide in heart failure patients.ESC Heart Fail. 2023 Dec;10(6):3250-3257. doi: 10.1002/ehf2.14542. Epub 2023 Sep 30. ESC Heart Fail. 2023. PMID: 37776150 Free PMC article. Review.
Cited by
-
Prognostic Value of Biomarkers in Cancer Patients Treated With Immune Checkpoint Inhibitor Therapy.JACC Adv. 2025 Jul 31;4(9):102022. doi: 10.1016/j.jacadv.2025.102022. Online ahead of print. JACC Adv. 2025. PMID: 40749516 Free PMC article.
References
-
- Echouffo‐Tcheugui JB, Shrader P, Thomas L, Gersh BJ, Kowey PR, Mahaffey KW, Singer DE, Hylek EM, Go AS, Peterson ED, Piccini JP, Fonarow GC. Care patterns and outcomes in atrial fibrillation patients with and without diabetes: ORBIT‐AF registry. J Am Coll Cardiol. 2017; 70: 1325–1335. - PubMed
-
- Santhanakrishnan R, Wang N, Larson MG, Magnani JW, McManus DD, Lubitz SA, Ellinor PT, Cheng S, Vasan RS, Lee DS, Wang TJ, Levy D, Benjamin EJ, Ho JE. Atrial fibrillation begets heart failure and vice versa: temporal associations and differences in preserved versus reduced ejection fraction. Circulation. 2016; 133: 484–492. - PMC - PubMed
-
- Vilain K, Li H, Kwong WJ, Antman EM, Ruff CT, Braunwald E, Cohen DJ, Giugliano RP, Magnuson EA, on behalf of the ENGAGE AF‐TIMI 48 Trial Investigators . Cardiovascular‐ and bleeding‐related hospitalization rates with edoxaban versus warfarin in patients with atrial fibrillation based on results of the ENGAGE AF‐TIMI 48 trial. Circ Cardiovasc Qual Outcomes. 2020; 13: e006511. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
