

One-year COVID-19 outcomes on the oncology care patient pathway: Results of a French descriptive, cross-sectional comprehensive study (ONCOCARE-COV)
- PMID: 35593199
- PMCID: PMC9348299
- DOI: 10.1002/cam4.4817
One-year COVID-19 outcomes on the oncology care patient pathway: Results of a French descriptive, cross-sectional comprehensive study (ONCOCARE-COV)
Abstract
Background: The COVID-19 pandemic led to a widely documented disruption in cancer care pathway. Since a resurgence of the pandemic was expected after the first lockdown in France, the global impact on the cancer care pathway over the year 2020 was investigated.
Aims: This study aimed to describe the changes in the oncology care pathway for cancer screening, diagnosis, assessment, diagnosis annoucement procedure and treatment over a one-year period.
Materials & methods: The ONCOCARE-COV study was a comprehensive, retrospective, descriptive, and cross-sectional study comparing the years 2019 and 2020. All key indicators along the cancer care pathway assessing the oncological activity over four periods were described. This study was set in a high-volume, public, single tertiary care center divided in two complementary sites (Reims University Hospital and Godinot Cancer Institute, Reims, France) which was located in a high COVID-19 incidence area during both peaks of the outbreak.
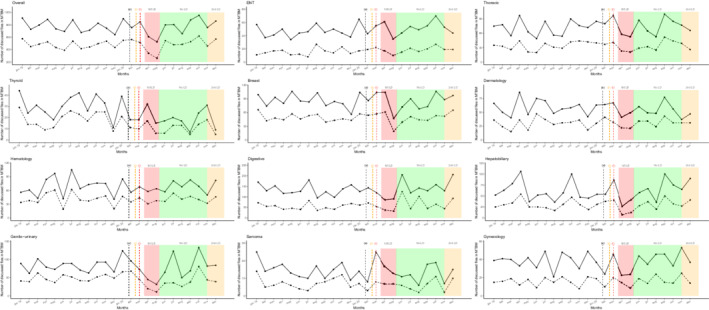
Results: A total of 26,566 patient's files were active during the year 2020. Breast screening (-19.5%), announcement dedicated consultations (-9.2%), Intravenous and Hyperthermic Intraoperative Intraperitoneal Chemotherapy (HIPECs) (-25%), and oncogeriatric evaluations (-14.8%) were heavily disrupted in regard to 2020 activity. We identified a clear second outbreak wave impact on medical announcement procedures (October, -14.4%), radiotherapy sessions (October, -16%), number of new health record discussed in multidisciplinary tumor board meeting (November, -14.6%) and HIPECs (November, -100%). Moreover, 2020 cancer care activity stagnated compared to 2019.
Discussion: The oncological care pathway was heavily disrupted during the first and second peaks of the COVID-19 outbreak. Between lockdowns, we observed a remarkable but non-compensatory recovery as well as a lesser impact from the pandemic resurgence. However, in absence of an increase in activity, a backlog persisted.
Conclusion: Public health efforts are needed to deal with the consequences of the COVID-19 pandemic on the oncology care pathway.
Keywords: COVID-19 pandemic; backlog; cancer care pathway; lockdowns.
© 2022 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Claire Carlier reported receiving honoraria as a speaker from Bristol Myers Squibb unrelated to this work. Damien Botsen reported receiving honoraria as a speaker and/or in an advisory role from Accord Healthcare, Amgen, Sanofi, Servier, and Pierre Fabre unrelated to this work. Florian Slimano reported receiving honoraria as a speaker and/or in an advisory role from Gilead, and Astra‐Zeneca unrelated to this work. Olivier Bouche reported receiving honoraria as a speaker and/or in an advisory role from Merck KGaA, Roche Genentech, Bayer, Astra‐Zeneca, Grunenthal, MSD, Amgen, Sanofi, Servier, and Pierre Fabre unrelated to this work. All other authors have no conflict of interest.
Figures


References
-
- Timeline: WHO's COVID‐19 response [Internet]. Accessed December 16, 2020. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019/interact...
-
- SPF . COVID‐19: point épidémiologique du 7 janvier 2021 [Internet]. Accessed February 23, 2021. https://www.santepubliquefrance.fr/maladies‐et‐traumatismes/maladies‐et‐...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
