

Sex and Age-Related Differences in Complement Factors Among Patients With Intermediate Age-Related Macular Degeneration
- PMID: 35594041
- PMCID: PMC9145081
- DOI: 10.1167/tvst.11.5.22
Sex and Age-Related Differences in Complement Factors Among Patients With Intermediate Age-Related Macular Degeneration
Abstract
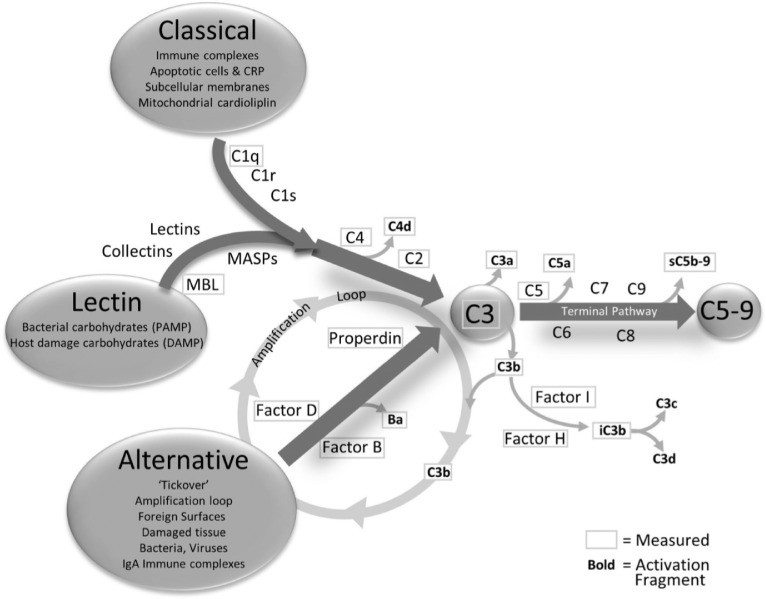
Purpose: Age-related macular degeneration (AMD) is an acquired degenerative disease of the retina classified into early, intermediate, and advanced AMD. A key factor in the pathogenesis of AMD is the complement system. The interaction of age and sex with the complement system may affect the risk of developing AMD. The purpose of this study was to determine if there were sex-specific differences in levels of complement factors among patients with the intermediate phenotype of AMD (iAMD) and explore the correlation between age and complement proteins.
Methods: We studied complement factors in patients with iAMD and controls without AMD. Nonparametric, rank-based linear regressions including a sex by AMD interaction were used to compare levels for each analyte. Correlations between age and complement proteins were evaluated using the Spearman rank correlation coefficient.
Results: We found significantly higher levels of factor B and factor I in females compared with males with iAMD, whereas no differences were seen in complement levels in male and female controls. The ratios of Ba/factor B, C3a/C3, C4b/C4, and C5a/C5 were not different in males and females with iAMD.
Conclusions: We demonstrate disparities in a subset of systemic complement factors between females and males with iAMD, but apparent complement turnover as measured by ratios of activation fragments to intact molecules was not different between these groups. The results suggest that complement system levels, including complement regulator factor I, exhibits sex-related differences in patients with iAMD and highlights that stratification by sex might be helpful in the interpretation of clinical trials of anticomplement therapy.
Conflict of interest statement
Disclosure:
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
