

Enhancing Radioiodine Incorporation into Radioiodine-Refractory Thyroid Cancer with MAPK Inhibition (ERRITI): A Single-Center Prospective Two-Arm Study
- PMID: 35594174
- PMCID: PMC9527501
- DOI: 10.1158/1078-0432.CCR-22-0437
Enhancing Radioiodine Incorporation into Radioiodine-Refractory Thyroid Cancer with MAPK Inhibition (ERRITI): A Single-Center Prospective Two-Arm Study
Abstract
Purpose: Restoration of iodine incorporation (redifferentiation) by MAPK inhibition was achieved in previously radioiodine-refractory, unresectable thyroid carcinoma (RR-TC). However, results were unsatisfactory in BRAFV600E-mutant (BRAF-MUT) RR-TC. Here we assess safety and efficacy of redifferentiation therapy through genotype-guided MAPK-modulation in patients with BRAF-MUT or wildtype (BRAF-WT) RR-TC.
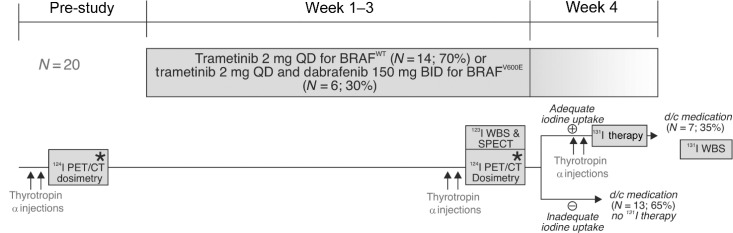
Patients and methods: In this prospective single-center, two-arm phase II study, patients received trametinib (BRAF-WT) or trametinib + dabrafenib (BRAF-MUT) for 21 ± 3 days. Redifferentiation was assessed by 123I-scintigraphy. In case of restored radioiodine uptake, 124I-guided 131I therapy was performed. Primary endpoint was the redifferentiation rate. Secondary endpoints were treatment response (thyroglobulin, RECIST 1.1) and safety. Parameters predicting successful redifferentiation were assessed using a receiver operating characteristic analysis and Youden J statistic.
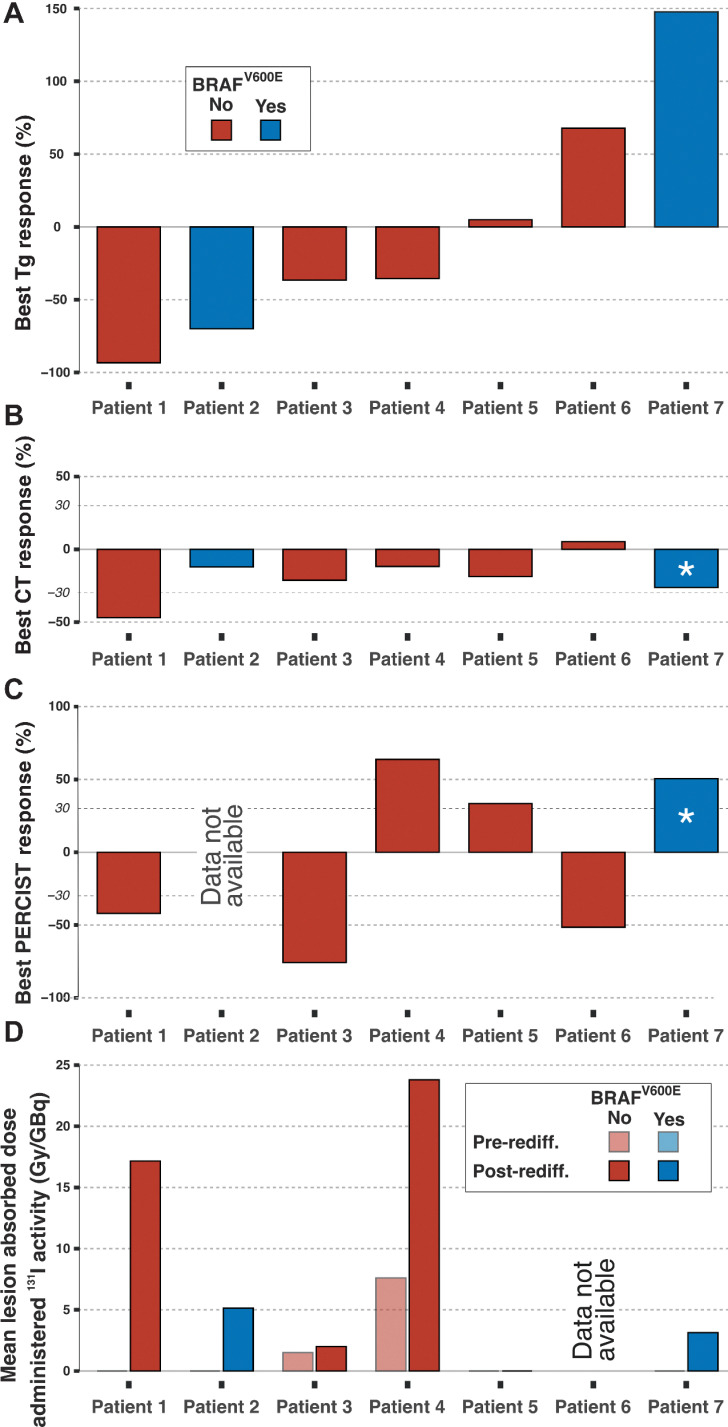
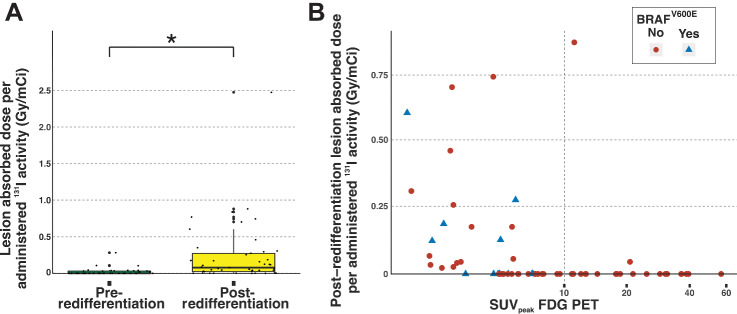
Results: Redifferentiation was achieved in 7 of 20 (35%) patients, 2 of 6 (33%) in the BRAF-MUT and 5 of 14 (36%) in the BRAF-WT arm. Patients received a mean (range) activity of 300.0 (273.0-421.6) mCi for 131I therapy. Any thyroglobulin decline was seen in 57% (4/7) of the patients, RECIST 1.1 stable/partial response/progressive disease in 71% (5/7)/14% (1/7)/14% (1/7). Peak standardized uptake value (SUVpeak) < 10 on 2[18F]fluoro-2-deoxy-D-glucose (FDG)-PET was associated with successful redifferentiation (P = 0.01). Transient pyrexia (grade 3) and rash (grade 4) were noted in one patient each.
Conclusions: Genotype-guided MAPK inhibition was safe and resulted in successful redifferentiation in about one third of patients in each arm. Subsequent 131I therapy led to a thyroglobulin (Tg) decline in more than half of the treated patients. Low tumor glycolytic rate as assessed by FDG-PET is predictive of redifferentiation success. See related commentary by Cabanillas et al., p. 4164.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
Redifferentiation Therapy-Returning to Our Roots in a Post-Kinase Inhibitor World.Clin Cancer Res. 2022 Oct 3;28(19):4164-4166. doi: 10.1158/1078-0432.CCR-22-1710. Clin Cancer Res. 2022. PMID: 35895318
References
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016;26:1–133. - PMC - PubMed
-
- Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab 2006;91:2892–9. - PubMed
-
- Schlumberger M, Brose M, Elisei R, Leboulleux S, Luster M, Pitoia F, et al. Definition and management of radioactive iodine-refractory differentiated thyroid cancer. Lancet Diabetes Endocrinol 2014;2:356–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
