

The Impact of Health Care Disparities on Patients With Heart Failure
- PMID: 35595161
- PMCID: PMC10289795
- DOI: 10.1016/j.cardfail.2022.04.008
The Impact of Health Care Disparities on Patients With Heart Failure
Abstract
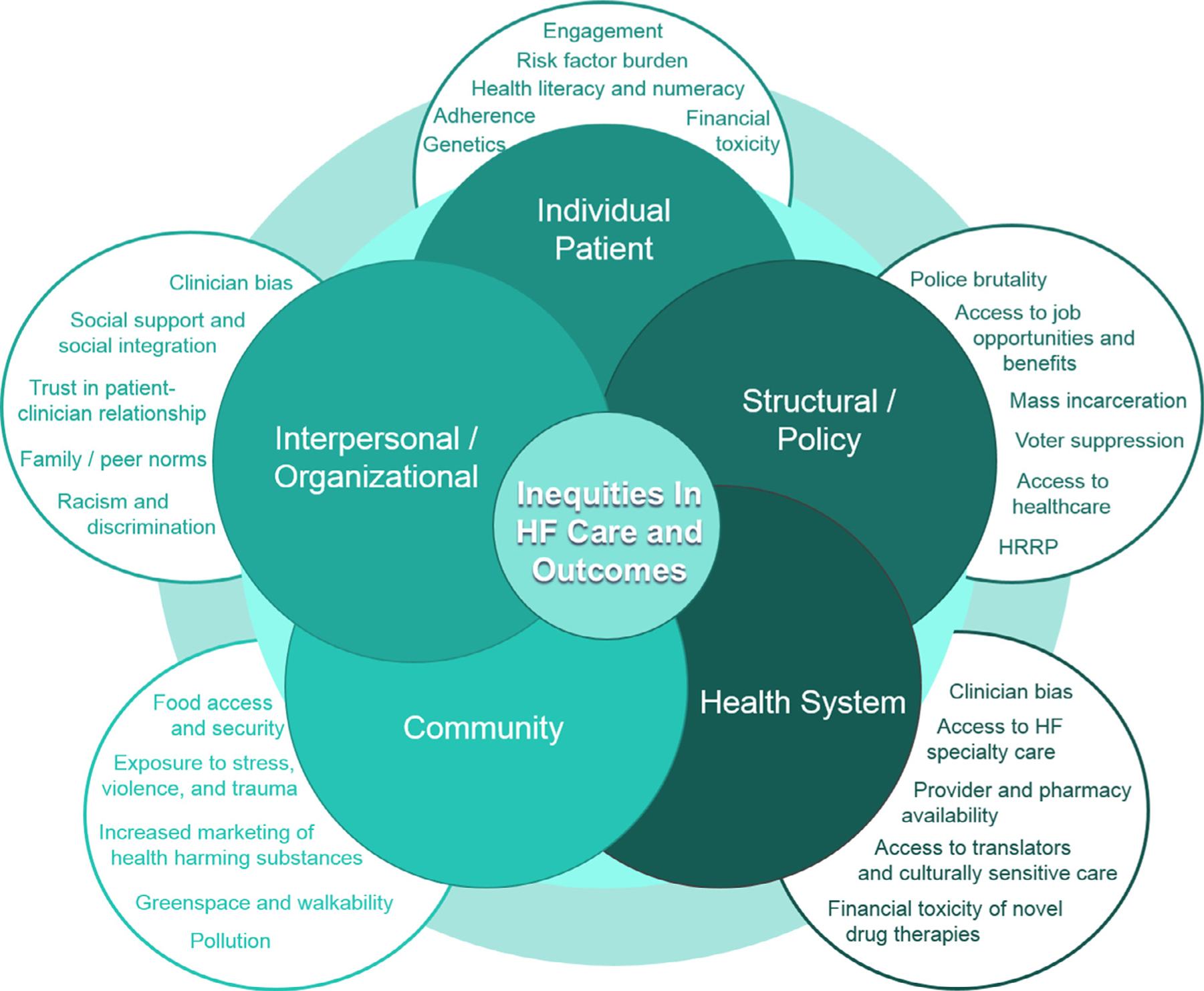
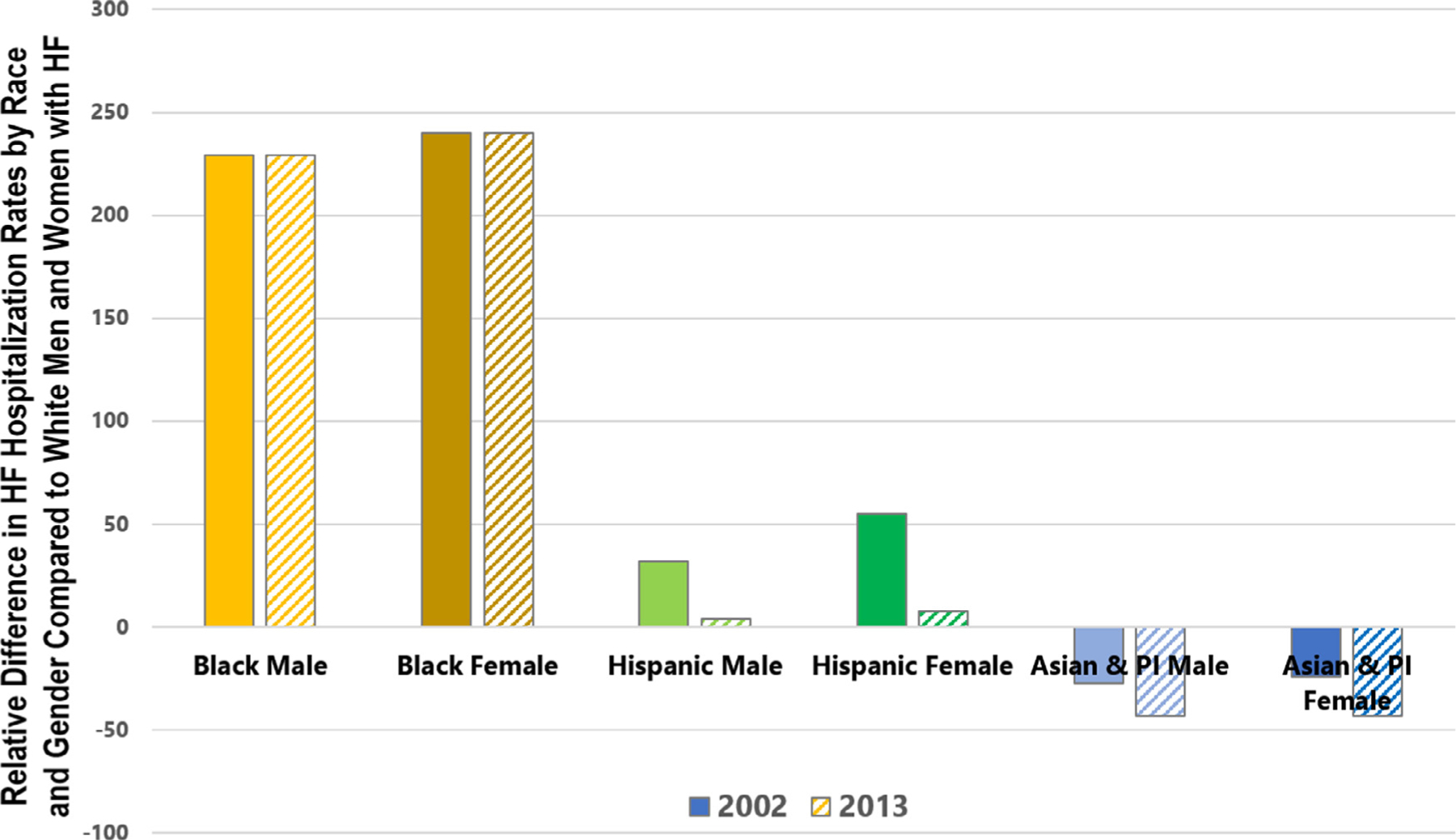
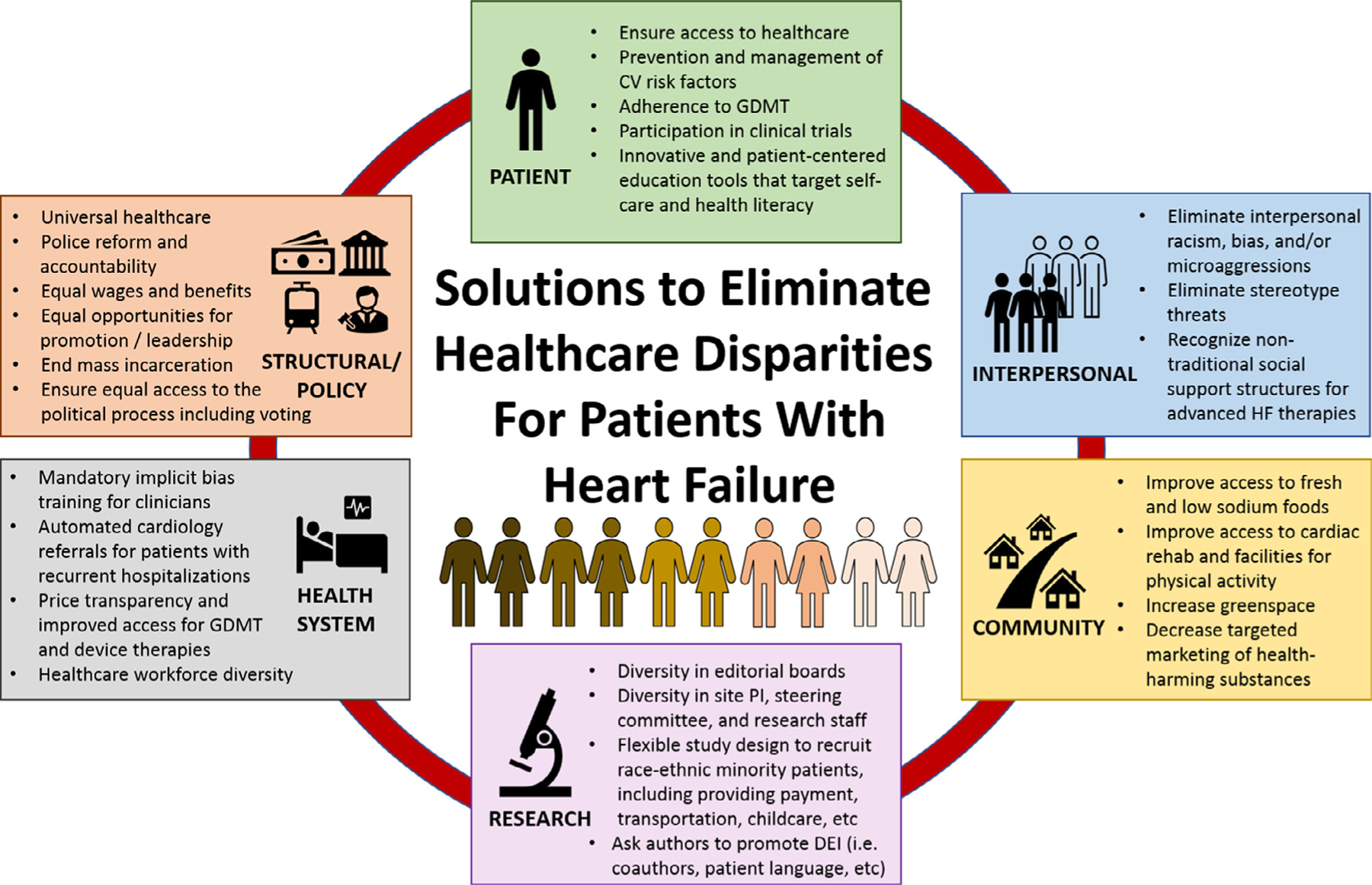
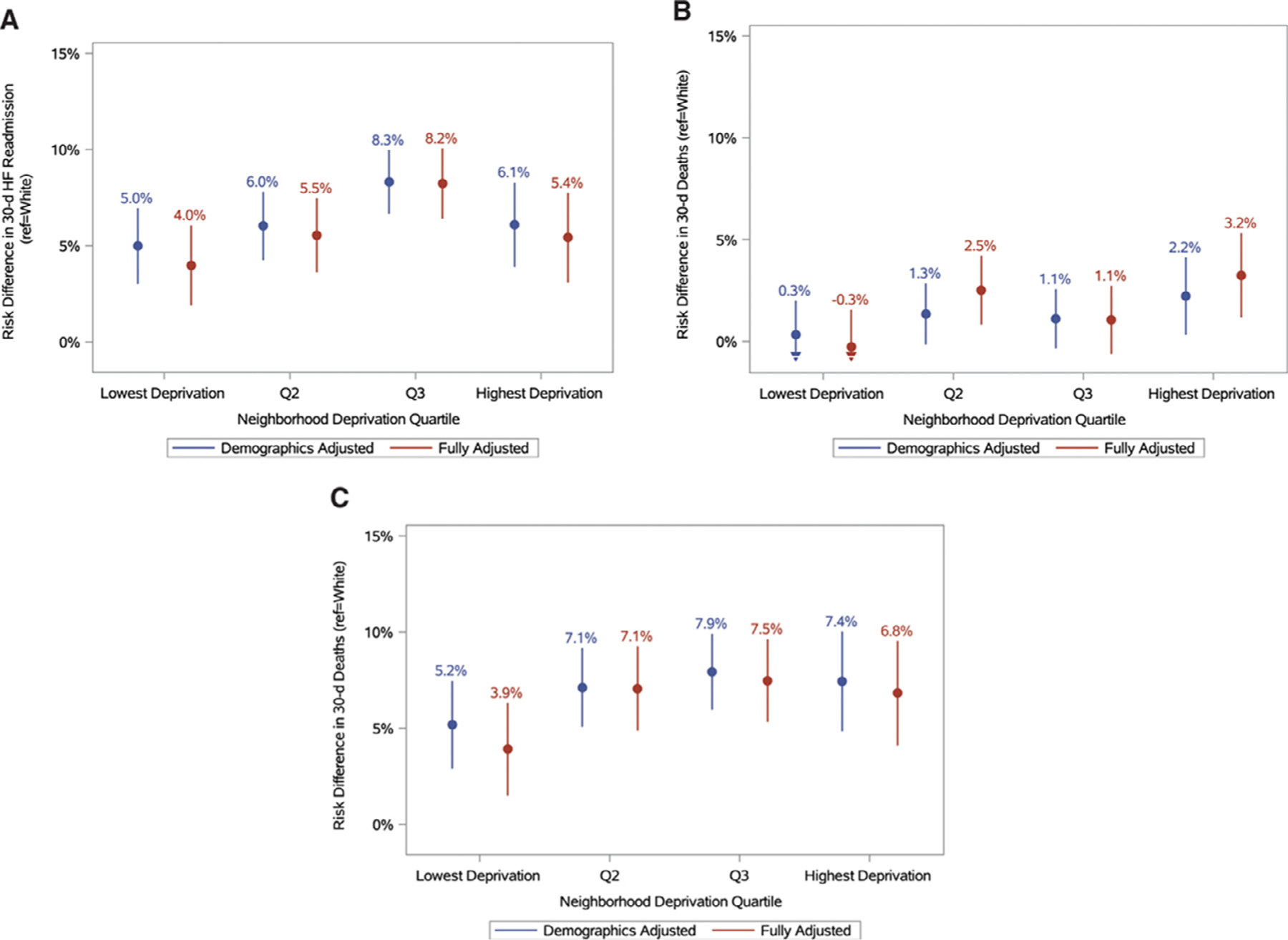
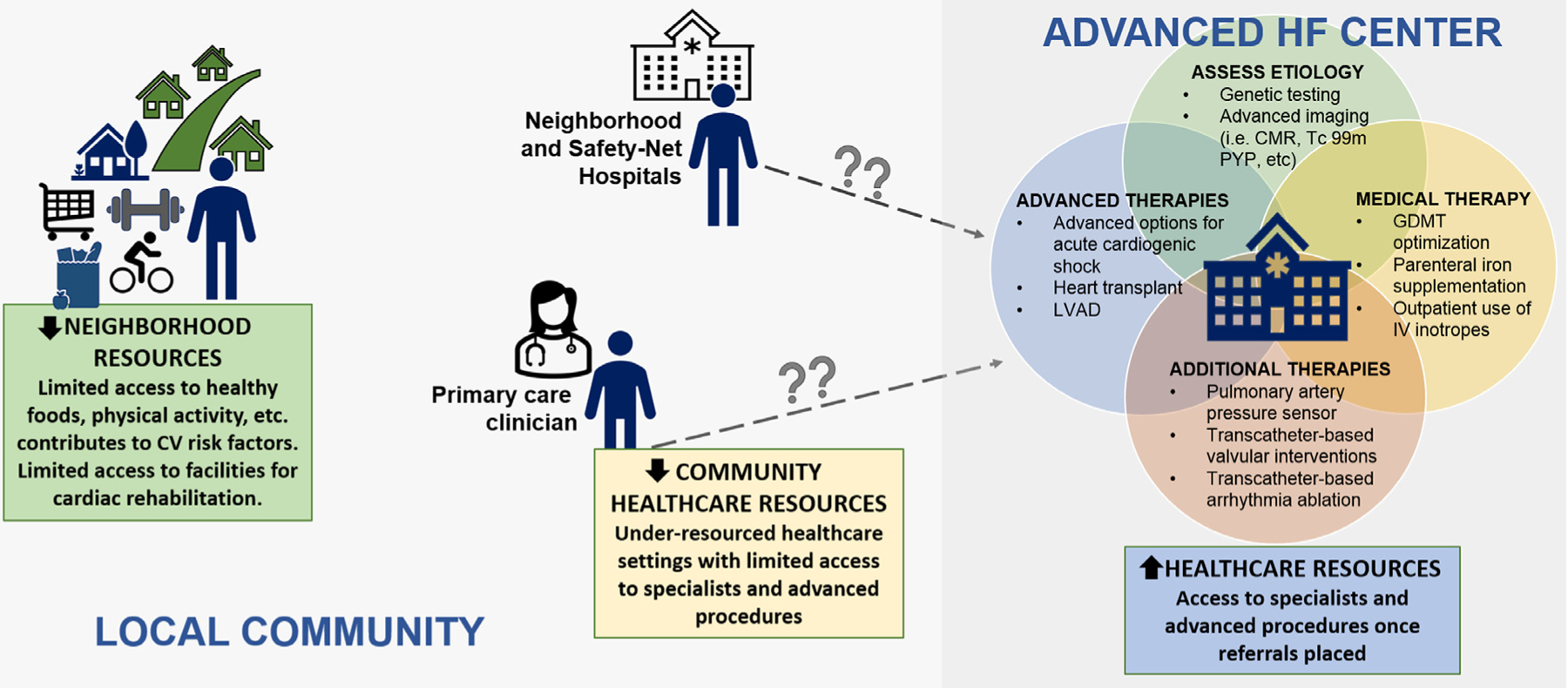
Heart failure (HF) remains a condition associated with high morbidity, mortality, and associated costs. Although the number of medical and device-based therapies available to treat HF are expanding at a remarkable rate, disparities in the risk for incident HF and treatments delivered to patients are also of growing concern. These disparities span across racial and ethnic groups, socioeconomic status, and apply across the spectrum of HF from stage A to stage D. The complexity of HF risk and treatment is further impacted by the number of patients who experience the downstream impact of social determinants of health. The purpose of this document is to highlight the known health care disparities that exist in the care of patients with HF and to provide a context for how clinicians and researchers should assess both biological and social determinants of HF risk in vulnerable populations. Furthermore, this document provides a framework for future steps that can be used to help diminish inequalities in access and clinical outcomes over time, and offer solutions to help decrease disparities within HF care.
Keywords: Heart failure; health care disparities; outcomes; race–ethnicity.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
