

Evolution of Investigating Informed Assent Discussions about CPR in Seriously Ill Patients
- PMID: 35595375
- PMCID: PMC9179950
- DOI: 10.1016/j.jpainsymman.2022.03.009
Evolution of Investigating Informed Assent Discussions about CPR in Seriously Ill Patients
Abstract
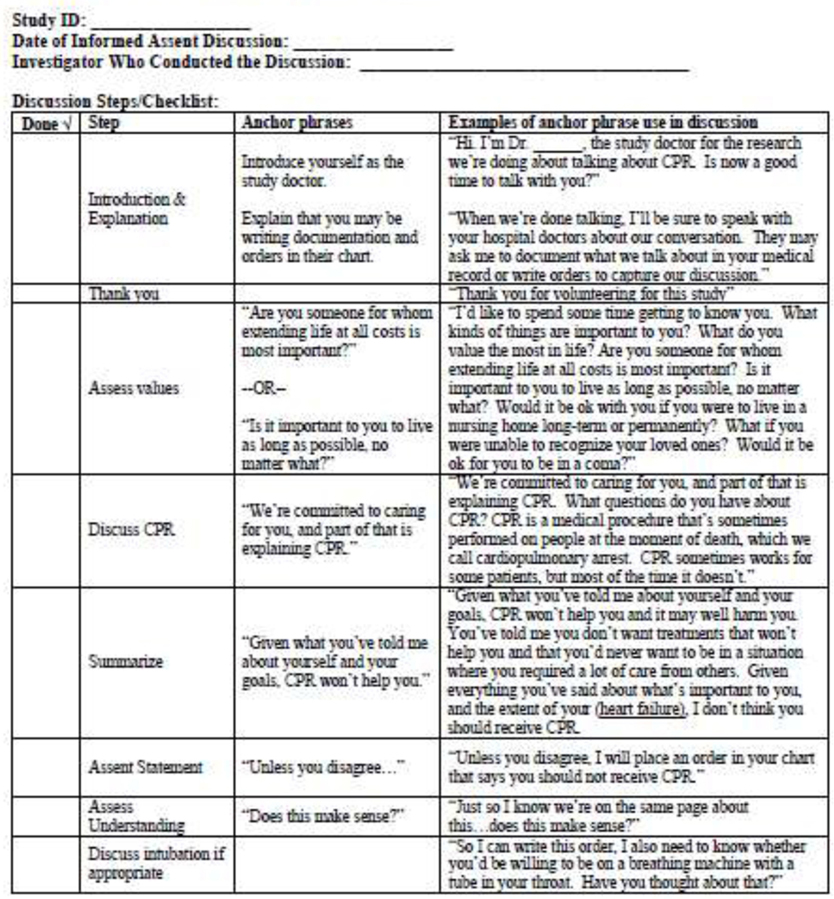
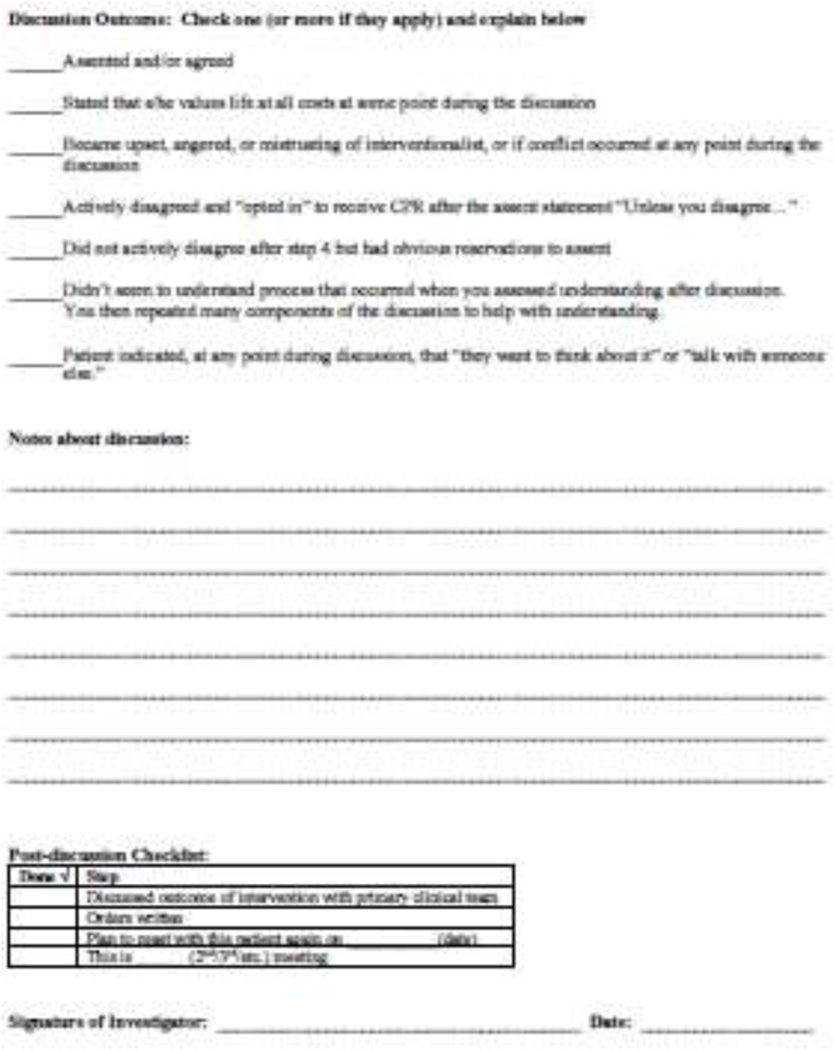
Context: Outcomes after cardiopulmonary resuscitation (CPR) remain poor. We have spent 10 years investigating an "informed assent" (IA) approach to discussing CPR with chronically ill patients/families. IA is a discussion framework whereby patients extremely unlikely to benefit from CPR are informed that unless they disagree, CPR will not be performed because it will not help achieve their goals, thus removing the burden of decision-making from the patient/family, while they retain an opportunity to disagree.
Objectives: Determine the acceptability and efficacy of IA discussions about CPR with older chronically ill patients/families.
Methods: This multi-site research occurred in three stages. Stage I determined acceptability of the intervention through focus groups of patients with advanced COPD or malignancy, family members, and physicians. Stage II was an ambulatory pilot randomized controlled trial (RCT) of the IA discussion. Stage III is an ongoing phase 2 RCT of IA versus attention control in in patients with advanced chronic illness.
Results: Our qualitative work found the IA approach was acceptable to most patients, families, and physicians. The pilot RCT demonstrated feasibility and showed an increase in participants in the intervention group changing from "full code" to "do not resuscitate" within two weeks after the intervention. However, Stages I and II found that IA is best suited to inpatients. Our phase 2 RCT in older hospitalized seriously ill patients is ongoing; results are pending.
Conclusions: IA is a feasible and reasonable approach to CPR discussions in selected patient populations.
Keywords: Code status; cardiopulmonary resuscitation; communication; end-of-life; seriously ill patients.
Copyright © 2022 American Academy of Hospice and Palliative Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- https://www.heart.org/en/professional/quality-improvement/get-with-the-g..., accessed Dec. 27, 2021.
-
- Schluep M, Gravesteijn BY, Stolker RJ, Endeman H, Hoeks SE. One-year survival after in-hospital cardiac arrest: A systematic review and meta-analysis. Resuscitation 2018;132:90–100. - PubMed
-
- Halpern SD, Ubel PA, Asch DA. Harnessing the power of default options to improve health care. N Engl J Med 2007;357:1340–4. - PubMed
