

Mechanical Circulatory Support: Primer for Consultant Specialists
- PMID: 35595531
- PMCID: PMC9269658
- DOI: 10.2215/CJN.13341021
Mechanical Circulatory Support: Primer for Consultant Specialists
Abstract
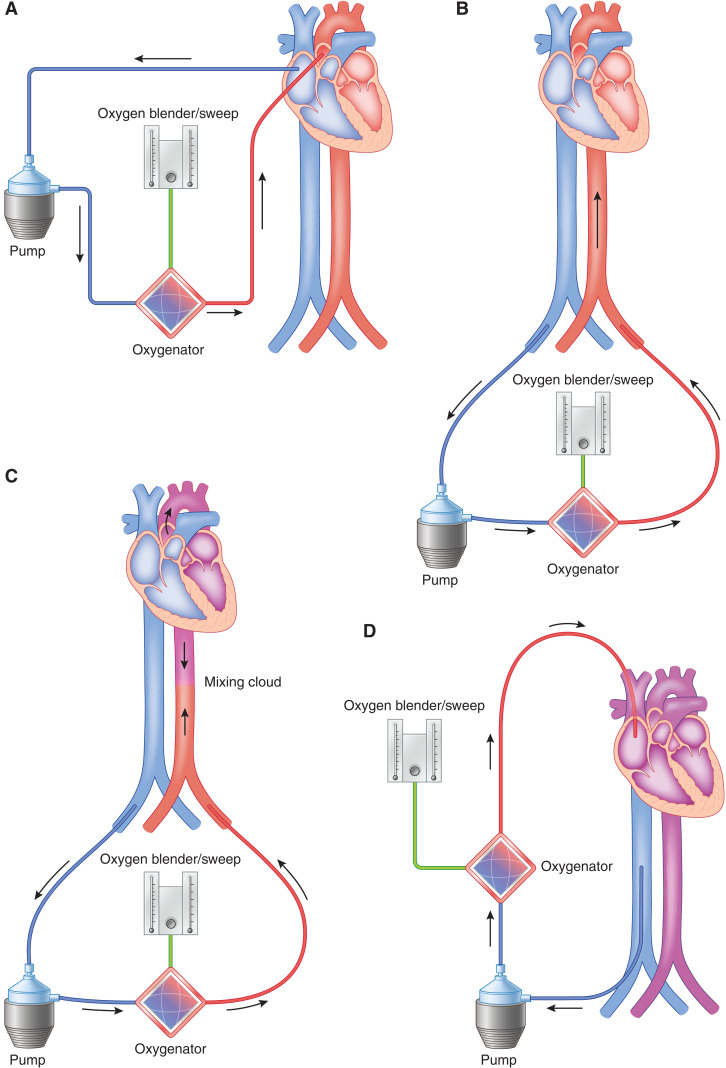
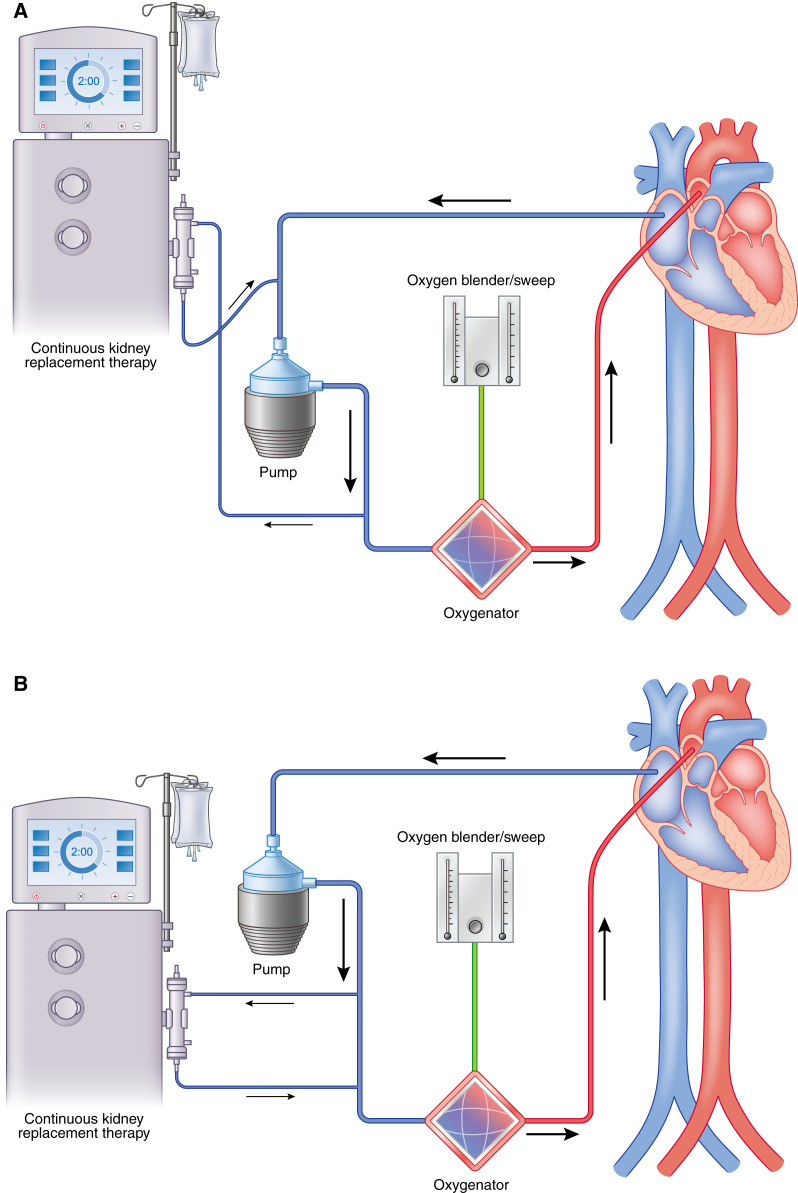
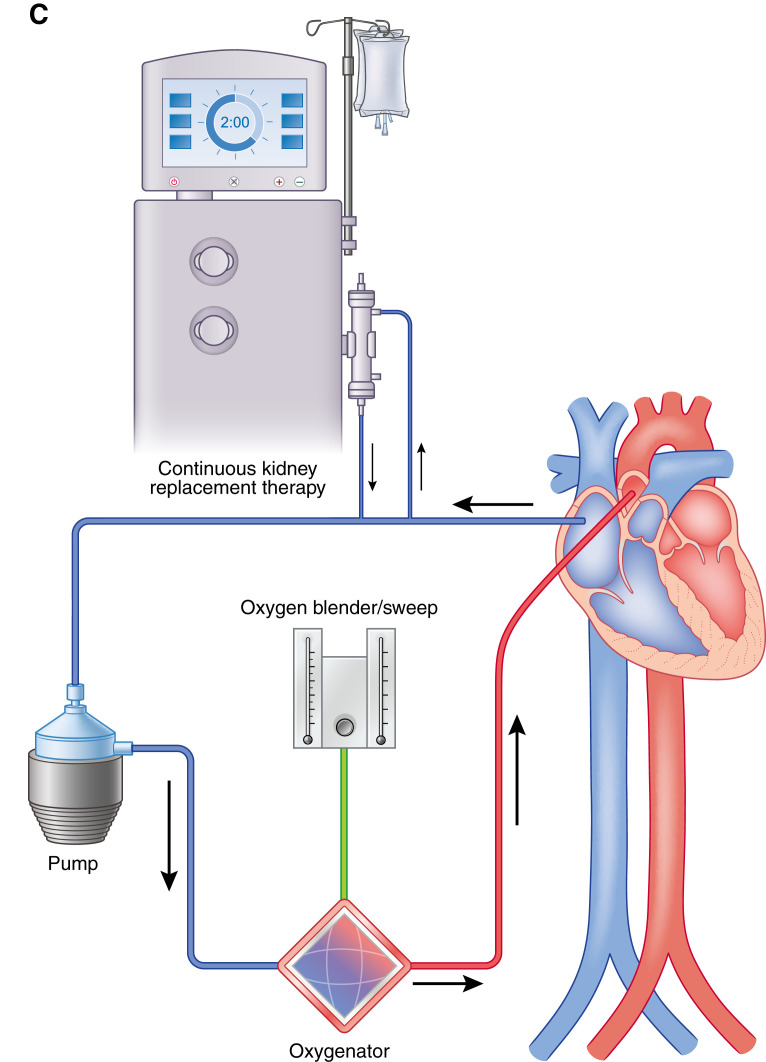
Mechanical life support therapies exist in many forms to temporarily replace the function of vital organs. Generally speaking, these tools are supportive therapy to allow for organ recovery but, at times, require transition to long-term mechanical support. This review will examine nonrenal extracorporeal life support for cardiac and pulmonary support as well as other mechanical circulatory support options. This is intended as a general primer and overview to assist nephrologist consultants participating in the care of these critically ill patients who often experience acute renal injury as a result of cardiopulmonary shock and from their exposure to mechanical circulatory support.
Keywords: cardiovascular; cardiovascular disease; critical care nephrology and acute kidney injury series; heart failure.
Copyright © 2022 by the American Society of Nephrology.
Figures
References
-
- Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, Richardt G, Hennersdorf M, Empen K, Fuernau G, Desch S, Eitel I, Hambrecht R, Fuhrmann J, Böhm M, Ebelt H, Schneider S, Schuler G, Werdan K; IABP-SHOCK II Trial Investigators : Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med 367: 1287–1296, 2012 - PubMed
-
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeJemtel TH: Early revascularization in acute myocardial infarction complicated by cardiogenic shock. N Engl J Med 341: 625–634, 1999 - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; ESC Scientific Document Group : 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure [published correction appears in Eur Heart J 2016;38:ehw383]. Eur Heart J 37: 2129–2200, 2016 - PubMed
-
- McMurray JJ, Pfeffer MA: Heart failure. Lancet 365: 1877–1889, 2005 - PubMed
-
- Tanai E, Frantz S: Pathophysiology of heart failure. Compr Physiol 6: 187–214, 2015 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
