

Three-dimensional finite element analysis of the effect of alveolar cleft bone graft on the maxillofacial biomechanical stabilities of unilateral complete cleft lip and palate
- PMID: 35596229
- PMCID: PMC9123812
- DOI: 10.1186/s12938-022-01000-y
Three-dimensional finite element analysis of the effect of alveolar cleft bone graft on the maxillofacial biomechanical stabilities of unilateral complete cleft lip and palate
Abstract
Background: The objective is to clarify the effect of alveolar cleft bone graft on maxillofacial biomechanical stabilities, the key areas when bone grafting and in which should be supplemented with bone graft once bone resorption occurred in UCCLP (unilateral complete cleft lip and palate).
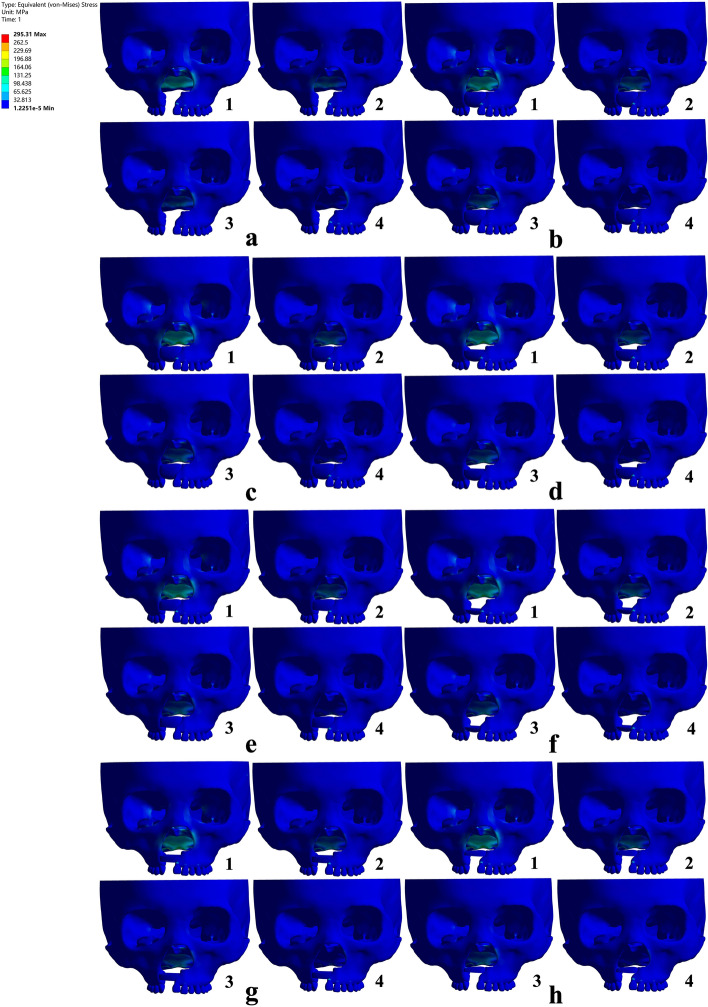
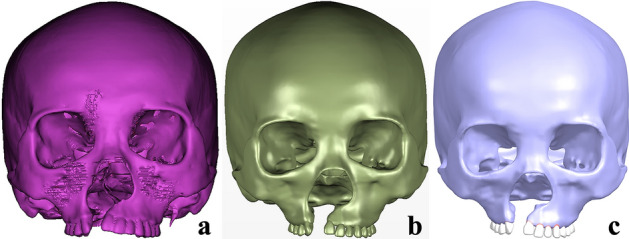
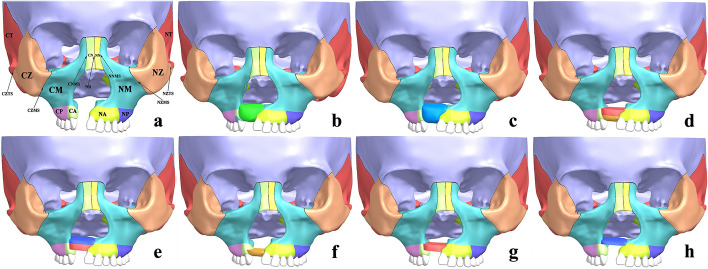
Methods: Maxillofacial CAD (computer aided design) models of non-bone graft and full maxilla cleft, full alveolar cleft bone graft, bone graft in other sites of the alveolar cleft were acquired by processing the UCCLP maxillofacial CT data in three-dimensional modeling software. The maxillofacial bone EQV (equivalent) stresses and bone suture EQV strains under occlusal states were obtained in the finite element analysis software.
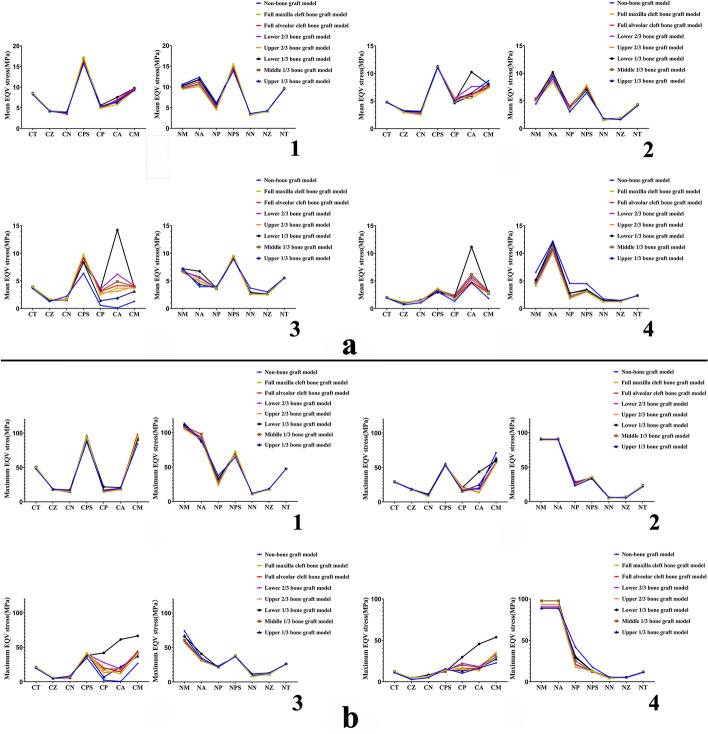
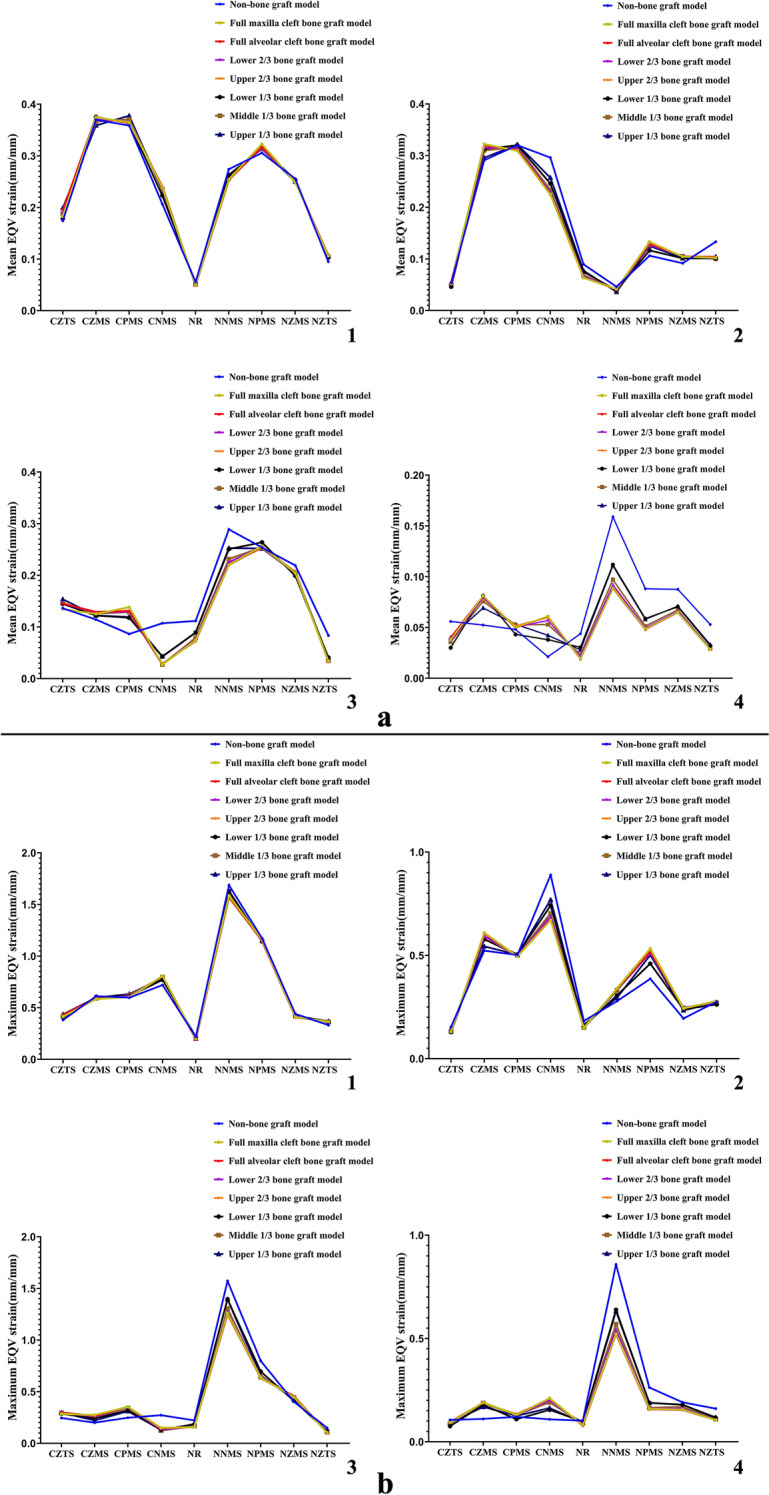
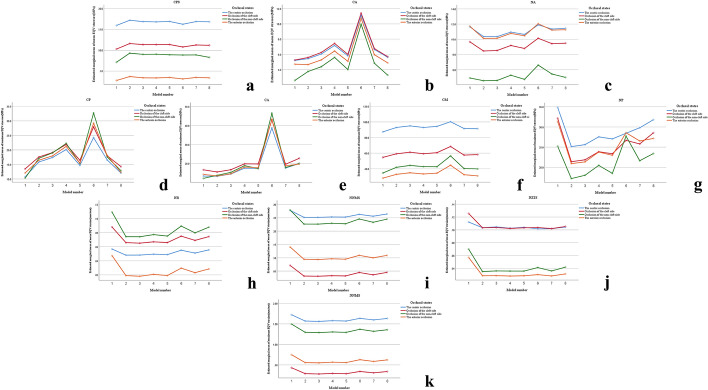
Results: Under corresponding occlusal states, the EQV stresses of maxilla, pterygoid process of sphenoid bone on the corresponding side and anterior alveolar arch on the non-cleft side were higher than other maxillofacial bones, the EQV strains of nasomaxillary, zygomaticomaxillary and pterygomaxillary suture on the corresponding side were higher than other maxillofacial bone sutures. The mean EQV strains of nasal raphe, the maximum EQV stresses of posterior alveolar arch on the non-cleft side, the mean and maximum EQV strains of nasomaxillary suture on the non-cleft side in full alveolar cleft bone graft model were all significantly lower than those in non-bone graft model. The mean EQV stresses of bilateral anterior alveolar arches, the maximum EQV stresses of maxilla and its alveolar arch on the cleft side in the model with bone graft in lower 1/3 of the alveolar cleft were significantly higher than those in full alveolar cleft bone graft model.
Conclusions: For UCCLP, bilateral maxillae, pterygoid processes of sphenoid bones and bilateral nasomaxillary, zygomaticomaxillary, pterygomaxillary sutures, anterior alveolar arch on the non-cleft side are the main occlusal load-bearing structures before and after alveolar cleft bone graft. Alveolar cleft bone graft mainly affects biomechanical stabilities of nasal raphe and posterior alveolar arch, nasomaxillary suture on the non-cleft side. The areas near nasal floor and in the middle of the alveolar cleft are the key sites when bone grafting, and should be supplemented with bone graft when the bone resorbed in these areas.
Keywords: Alveolar cleft bone graft; Equivalent strain; Equivalent stress; Maxillofacial bone; Maxillofacial bone suture; Unilateral complete cleft lip and palate.
© 2022. The Author(s).
Conflict of interest statement
There are no competing interests in the research.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
