

Clinical and organizational factors associated with mortality during the peak of first COVID-19 wave: the global UNITE-COVID study
- PMID: 35596752
- PMCID: PMC9123859
- DOI: 10.1007/s00134-022-06705-1
Clinical and organizational factors associated with mortality during the peak of first COVID-19 wave: the global UNITE-COVID study
Erratum in
-
Correction to: Clinical and organizational factors associated with mortality during the peak of first COVID-19 wave: the global UNITE-COVID study.Intensive Care Med. 2022 Aug;48(8):1130-1131. doi: 10.1007/s00134-022-06801-2. Intensive Care Med. 2022. PMID: 35796813 Free PMC article. No abstract available.
Abstract
Purpose: To accommodate the unprecedented number of critically ill patients with pneumonia caused by coronavirus disease 2019 (COVID-19) expansion of the capacity of intensive care unit (ICU) to clinical areas not previously used for critical care was necessary. We describe the global burden of COVID-19 admissions and the clinical and organizational characteristics associated with outcomes in critically ill COVID-19 patients.
Methods: Multicenter, international, point prevalence study, including adult patients with SARS-CoV-2 infection confirmed by polymerase chain reaction (PCR) and a diagnosis of COVID-19 admitted to ICU between February 15th and May 15th, 2020.
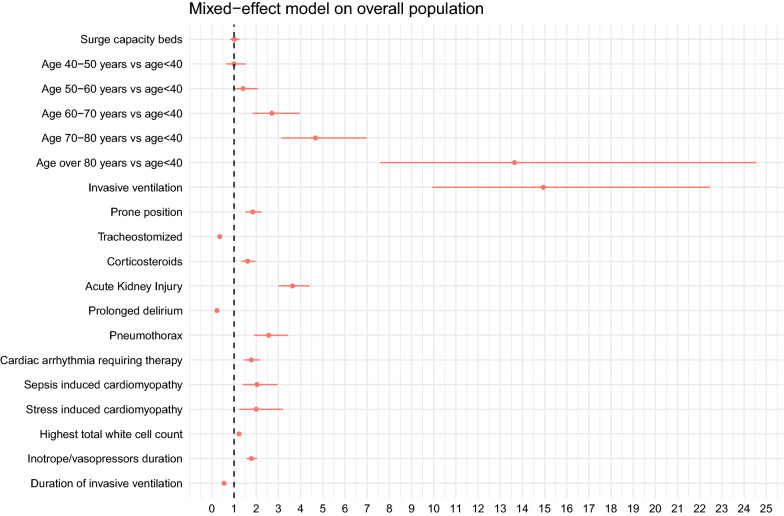
Results: 4994 patients from 280 ICUs in 46 countries were included. Included ICUs increased their total capacity from 4931 to 7630 beds, deploying personnel from other areas. Overall, 1986 (39.8%) patients were admitted to surge capacity beds. Invasive ventilation at admission was present in 2325 (46.5%) patients and was required during ICU stay in 85.8% of patients. 60-day mortality was 33.9% (IQR across units: 20%-50%) and ICU mortality 32.7%. Older age, invasive mechanical ventilation, and acute kidney injury (AKI) were associated with increased mortality. These associations were also confirmed specifically in mechanically ventilated patients. Admission to surge capacity beds was not associated with mortality, even after controlling for other factors.
Conclusions: ICUs responded to the increase in COVID-19 patients by increasing bed availability and staff, admitting up to 40% of patients in surge capacity beds. Although mortality in this population was high, admission to a surge capacity bed was not associated with increased mortality. Older age, invasive mechanical ventilation, and AKI were identified as the strongest predictors of mortality.
Keywords: COVID-19; Critical care; Pneumonia; SARS-CoV-2; Surge capacity.
© 2022. The Author(s).
Conflict of interest statement
AE, FD, GDP, LG, VG, AJ, JK, AL, JM, SNM, MO, MP, MC declare no conflicts of interest. MG reports speaking fees from Baxter and Philips. TDC is supported by Research Foundation Flanders (Grant nr G085920N). MA reports Research Grant from GE, Honoraria from Fisher and Paykel, Pfizer, Orion and Gilead. GC reports grants, personal fees as Speakers’ Bureau Member and Advisory Board Member from Integra and Neuroptics, all outside the submitted work. ACM is supported by a Clinician Scientist Fellowship from the Medical Research Council (MR/V006118/1). SE declares no financial COIs and the following non-financial disclosures: Cochrane editor, American Society of Anesthesiologist data review board member. LF reports research funding from NIHR, Baxter, Ortho-Clinical Diagnostics, Exthera Medical and lecture fees from Baxter, Fresenius, Paion, all outside the submitted work. GG received payment for lectures from Getinge, Draeger Medical, Fisher&Paykel, Biotest, MSD, Gilead and unrestricted research grants from Fisher&Paykel and MSD (all unrelated to the present work). MCMD declares potential conflict of interest with BD. PP declares potential conflicts of interest with Pfizer, MSD and Gilead. SJS reports personal fees from Springer-Verlag, GmbH (Vienna, Austria) for educational commitments grants and non-financial support from ESICM (Bruxelles, Belgium), Fresenius (Germany), Liberate Medical LLC (Crestwood, USA), STIMIT AG (Nidau, Switzerland) Reactive Robotics GmbH (Munich, Germany) as well as from Technical University of Munich, Germany, from national (e.g. DGAI) and international (e.g. ESICM) medical societies (or their congress organizers) in the field of anesthesiology and intensive care, all outside the submitted work; SJS holds stocks in small amounts from Alphabeth Inc., Bayer AG, Rhön-Klinikum AG, and Siemens AG. These did not have any influence on this study. AW reports Honorarium for delivery of educational material for Vygon, GE. JLT declares potential conflict of interest with Getinge. JDW has consulted for Pfizer, MSD (honoraria paid to institution), and is a senior clinical investigator funded by the Research Foundation Flanders (FWO, Ref. 1881020N).
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
