

Comparison of different metrics of cerebral autoregulation in association with major morbidity and mortality after cardiac surgery
- PMID: 35597624
- PMCID: PMC9428920
- DOI: 10.1016/j.bja.2022.03.029
Comparison of different metrics of cerebral autoregulation in association with major morbidity and mortality after cardiac surgery
Abstract
Background: Cardiac surgery studies have established the clinical relevance of personalised arterial blood pressure management based on cerebral autoregulation. However, variabilities exist in autoregulation evaluation. We compared the association of several cerebral autoregulation metrics, calculated using different methods, with outcomes after cardiac surgery.
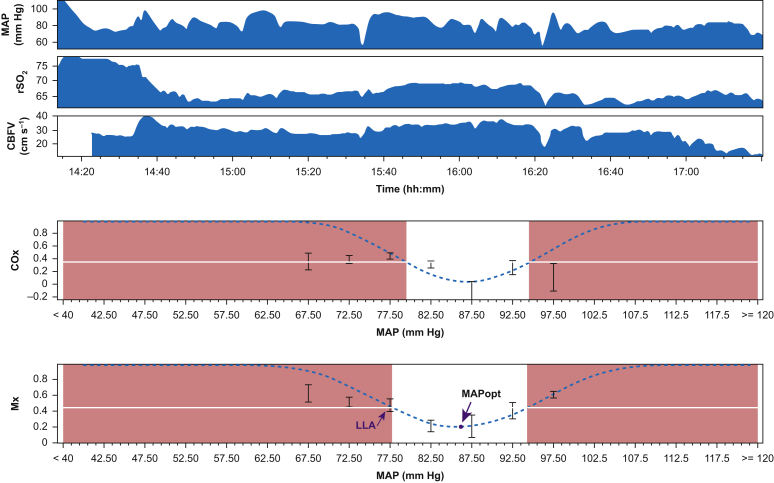
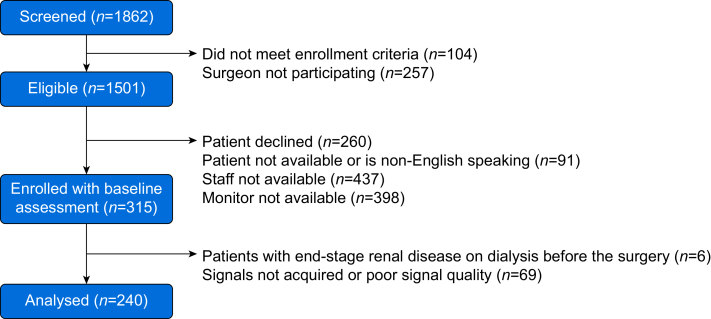
Methods: Autoregulation was measured during cardiac surgery in 240 patients. Mean flow index and cerebral oximetry index were calculated as Pearson's correlations between mean arterial pressure (MAP) and transcranial Doppler blood flow velocity or near-infrared spectroscopy signals. The lower limit of autoregulation and optimal mean arterial pressure were identified using mean flow index and cerebral oximetry index. Regression models were used to examine associations of area under curve and duration of mean arterial pressure below thresholds with stroke, acute kidney injury (AKI), and major morbidity and mortality.
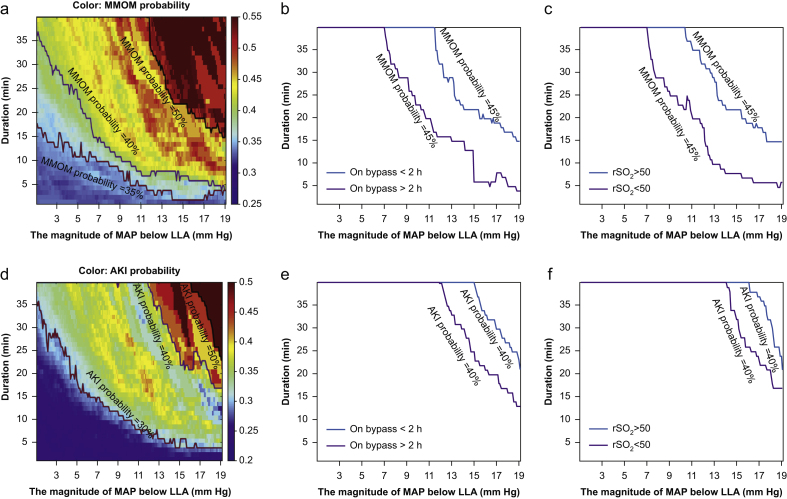
Results: Both mean flow index and cerebral oximetry index identified the cerebral lower limit of autoregulation below which MAP was associated with a higher incidence of AKI and major morbidity and mortality. Based on magnitude and significance of the estimates in adjusted models, the area under curve of MAP < lower limit of autoregulation had the strongest association with AKI and major morbidity and mortality. The odds ratio for area under the curve of MAP < lower limit of autoregulation was 1.05 (95% confidence interval, 1.01-1.09), meaning every 1 mm Hg h increase of area under the curve was associated with an average increase in the odds of AKI by 5%.
Conclusions: For cardiac surgery patients, area under curve of MAP < lower limit of autoregulation using mean flow index or cerebral oximetry index had the strongest association with AKI and major morbidity and mortality. Trials are necessary to evaluate this target for MAP management.
Keywords: acute kidney injury; cardio pulmonary bypass; cerebral autoregulation; data visualisation; individualised blood pressure management; major morbidity, mortality; organ injury; postoperative outcome.
Copyright © 2022 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declarations of interest CHB reported receiving grants from the National Institutes of Health (NIH) during the conduct of the study, and consulting for and participating in a data share with Medtronic. CWH reported receiving grants and personal fees for being a consultant and providing lectures for Medtronic/Covidien, Inc., being a consultant to Merck, Inc., and receiving grants from the NIH outside of the submitted work. JKL has received support from and been a paid consultant for Medtronic, and she is a paid consultant Edwards Life Sciences. JKL arrangements have been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies. Some methods used to measure and monitor autoregulation as described in this manuscript were patented by The Johns Hopkins University, listing KMB as a co-inventor. These patents are exclusively licensed to Medtronic Inc., and KMB received a portion of the licensing fee. PS and MC are authors of ICM+ software licensed by Cambridge Enterprise Ltd, UK, and have a financial interest in a part of licensing fee.
Figures
Similar articles
-
Determining Thresholds for Three Indices of Autoregulation to Identify the Lower Limit of Autoregulation During Cardiac Surgery.Crit Care Med. 2021 Apr 1;49(4):650-660. doi: 10.1097/CCM.0000000000004737. Crit Care Med. 2021. PMID: 33278074 Free PMC article.
-
Duration and magnitude of blood pressure below cerebral autoregulation threshold during cardiopulmonary bypass is associated with major morbidity and operative mortality.J Thorac Cardiovasc Surg. 2014 Jan;147(1):483-9. doi: 10.1016/j.jtcvs.2013.07.069. Epub 2013 Sep 26. J Thorac Cardiovasc Surg. 2014. PMID: 24075467 Free PMC article.
-
Predicting the limits of cerebral autoregulation during cardiopulmonary bypass.Anesth Analg. 2012 Mar;114(3):503-10. doi: 10.1213/ANE.0b013e31823d292a. Epub 2011 Nov 21. Anesth Analg. 2012. PMID: 22104067 Free PMC article.
-
Journal of clinical monitoring and computing 2016 end of year summary: monitoring cerebral oxygenation and autoregulation.J Clin Monit Comput. 2017 Apr;31(2):241-246. doi: 10.1007/s10877-017-9980-7. Epub 2017 Jan 24. J Clin Monit Comput. 2017. PMID: 28120178 Free PMC article. Review.
-
Monitoring of cerebral blood flow autoregulation: physiologic basis, measurement, and clinical implications.Br J Anaesth. 2024 Jun;132(6):1260-1273. doi: 10.1016/j.bja.2024.01.043. Epub 2024 Mar 12. Br J Anaesth. 2024. PMID: 38471987 Review.
Cited by
-
Quick Assessment of the Lower Limit of Cerebral Autoregulation Using Transcranial Doppler during Cardiopulmonary Bypass in Cardiac Surgery: A Feasibility Study.Rev Cardiovasc Med. 2023 May 31;24(6):156. doi: 10.31083/j.rcm2406156. eCollection 2023 Jun. Rev Cardiovasc Med. 2023. PMID: 39077528 Free PMC article.
-
The Conundrum of Systemic Arterial Pressure Management on Cardiopulmonary Bypass.J Clin Med. 2023 Jan 19;12(3):806. doi: 10.3390/jcm12030806. J Clin Med. 2023. PMID: 36769463 Free PMC article.
-
The importance of monitoring cerebral oxygenation in non brain injured patients.J Clin Monit Comput. 2023 Aug;37(4):943-949. doi: 10.1007/s10877-023-01002-8. Epub 2023 Apr 12. J Clin Monit Comput. 2023. PMID: 37043157 Free PMC article. Review.
-
Cerebral autoregulation monitoring in neonates and infants after cardiac surgery with cardiopulmonary bypass - comparison of single ventricle and biventricular physiology.Front Pediatr. 2025 Mar 28;13:1540870. doi: 10.3389/fped.2025.1540870. eCollection 2025. Front Pediatr. 2025. PMID: 40224386 Free PMC article.
-
Time-domain methods for quantifying dynamic cerebral blood flow autoregulation: Review and recommendations. A white paper from the Cerebrovascular Research Network (CARNet).J Cereb Blood Flow Metab. 2024 Sep;44(9):1480-1514. doi: 10.1177/0271678X241249276. Epub 2024 Apr 30. J Cereb Blood Flow Metab. 2024. PMID: 38688529 Free PMC article. Review.
References
-
- Czosnyka M., Smielewski P., Kirkpatrick P., Menon D.K., Pickard J.D. Monitoring of cerebral autoregulation in head-injured patients. Stroke. 1996;27:1829–1834. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
