

Indocyanine green fluorescence image processing techniques for breast cancer macroscopic demarcation
- PMID: 35597783
- PMCID: PMC9124184
- DOI: 10.1038/s41598-022-12504-x
Indocyanine green fluorescence image processing techniques for breast cancer macroscopic demarcation
Abstract
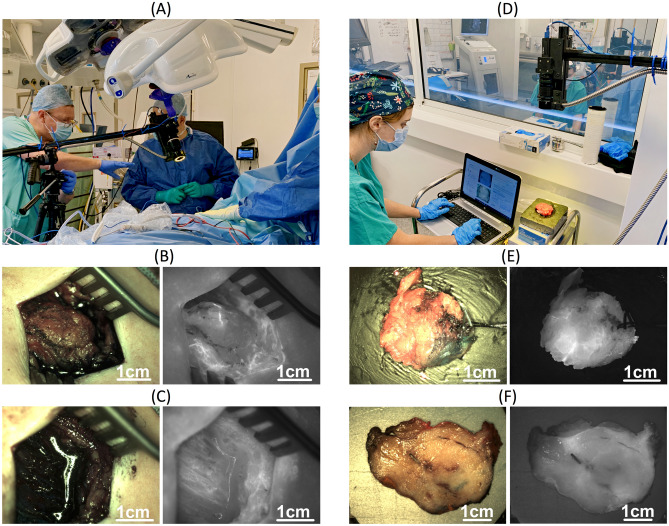
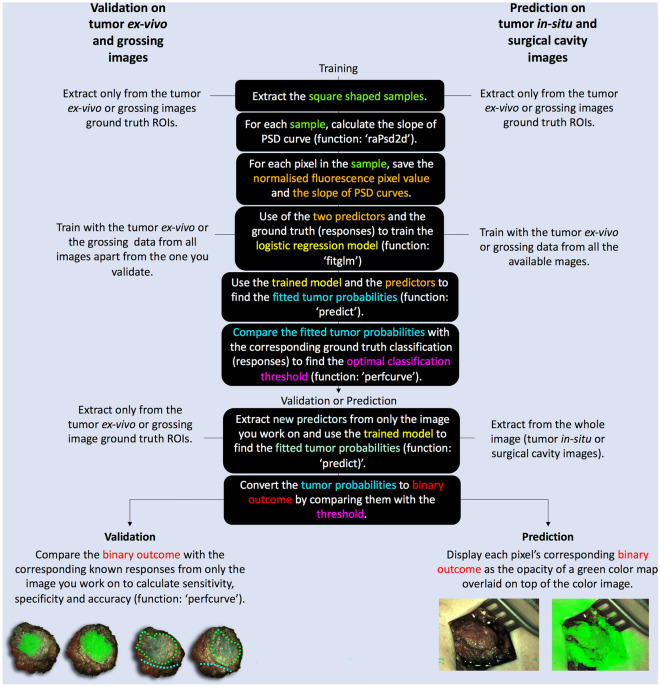
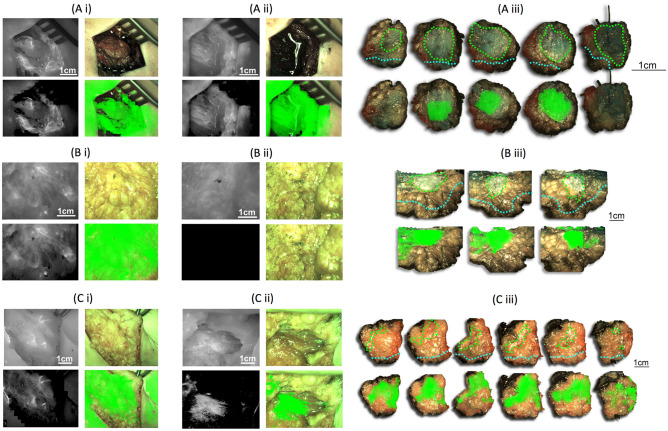
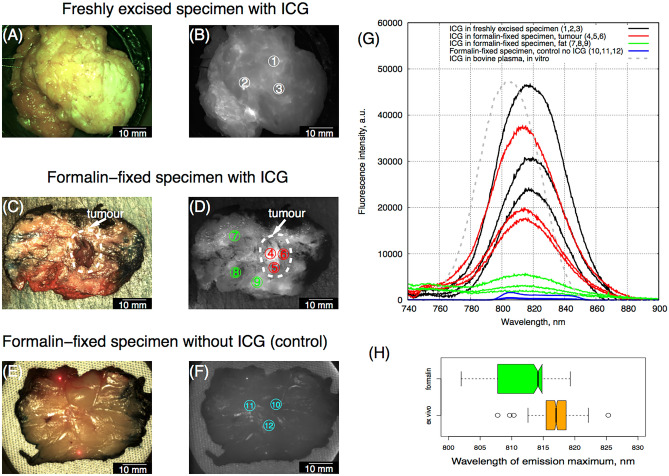
Re-operation due to disease being inadvertently close to the resection margin is a major challenge in breast conserving surgery (BCS). Indocyanine green (ICG) fluorescence imaging could be used to visualize the tumor boundaries and help surgeons resect disease more efficiently. In this work, ICG fluorescence and color images were acquired with a custom-built camera system from 40 patients treated with BCS. Images were acquired from the tumor in-situ, surgical cavity post-excision, freshly excised tumor and histopathology tumour grossing. Fluorescence image intensity and texture were used as individual or combined predictors in both logistic regression (LR) and support vector machine models to predict the tumor extent. ICG fluorescence spectra in formalin-fixed histopathology grossing tumor were acquired and analyzed. Our results showed that ICG remains in the tissue after formalin fixation. Therefore, tissue imaging could be validated in freshly excised and in formalin-fixed grossing tumor. The trained LR model with combined fluorescence intensity (pixel values) and texture (slope of power spectral density curve) identified the tumor's extent in the grossing images with pixel-level resolution and sensitivity, specificity of 0.75 ± 0.3, 0.89 ± 0.2.This model was applied on tumor in-situ and surgical cavity (post-excision) images to predict tumor presence.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Ye JC, Yan W, Christos PJ, Nori D, Ravi A. Equivalent survival with mastectomy or breast conserving surgery plus radiation in young women under the age of 40 with early-stage breast cancer: a national registry based stage-by-stage comparison. Clin. Breast Cancer. 2015;15:390–397. doi: 10.1016/j.clbc.2015.03.012. - DOI - PMC - PubMed
-
- Moyer, A. in Psychosocial outcomes of breast-conserving surgery versus mastectomy: A meta-analytic review 288 (American Psychological Association, Washington, DC, US, 1999). - PubMed
-
- MacNeill, F. & Irvine, T. Breast Surgery GIRFT Programme National Specialty Report, (2021).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
