

Feasibility and acceptability of high-intensity interval training and moderate-intensity continuous training in kidney transplant recipients: the PACE-KD study
- PMID: 35597974
- PMCID: PMC9123685
- DOI: 10.1186/s40814-022-01067-3
Feasibility and acceptability of high-intensity interval training and moderate-intensity continuous training in kidney transplant recipients: the PACE-KD study
Abstract
Background: Kidney transplant recipients (KTRs) exhibit unique elevated inflammation, impaired immune function, and increased cardiovascular risk. Although exercise reduces cardiovascular risk, there is limited research on this population, particularly surrounding novel high-intensity interval training (HIIT). The purpose of this pilot study was to determine the feasibility and acceptability of HIIT in KTRs.
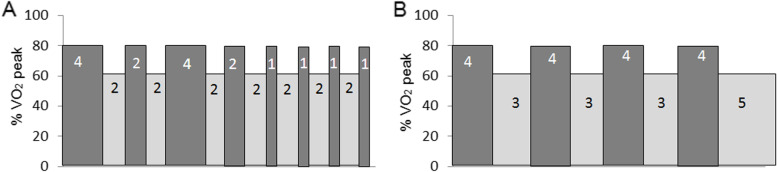
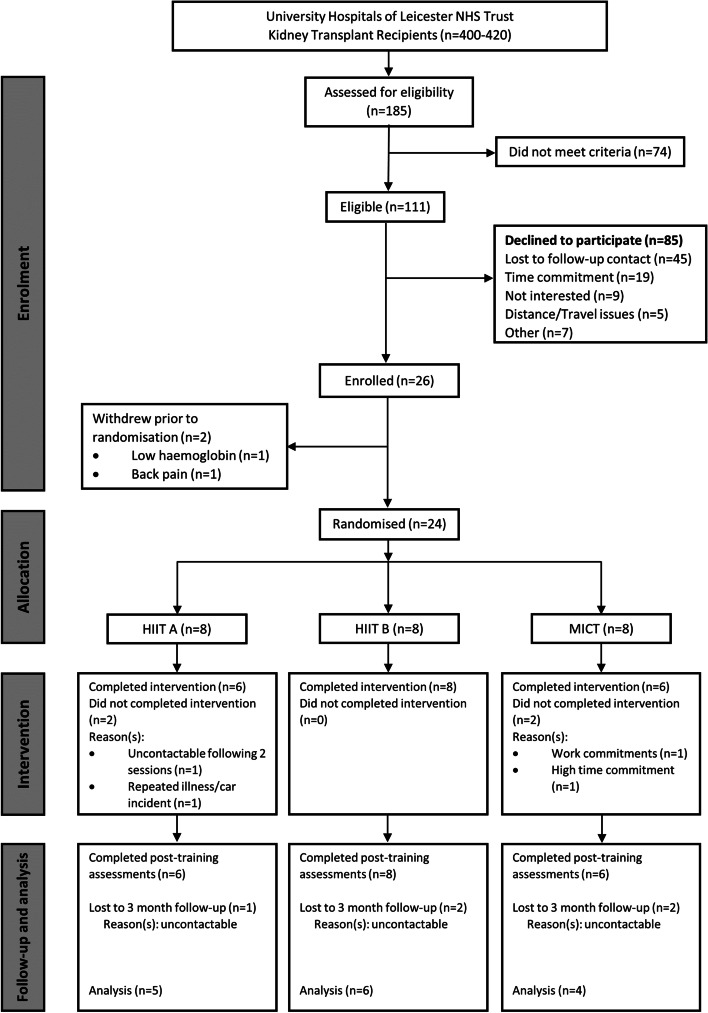
Methods: Twenty KTRs (male 14; eGFR 58±19 mL/min/1.73 m2; age 49±11 years) were randomised and completed one of three trials: HIIT A (4-, 2-, and 1-min intervals; 80-90% watts at V̇O2peak), HIITB (4×4 min intervals; 80-90% V̇O2peak) or MICT (~40 min; 50-60% V̇O2peak) for 24 supervised sessions on a stationary bike (approx. 3x/week over 8 weeks) and followed up for 3 months. Feasibility was assessed by recruitment, retention, and intervention acceptability and adherence.
Results: Twenty participants completed the intervention, and 8 of whom achieved the required intensity based on power output (HIIT A, 0/6 [0%]; HIITB, 3/8 [38%]; MICT, 5/6 [83%]). Participants completed 92% of the 24 sessions with 105 cancelled and rescheduled sessions and an average of 10 weeks to complete the intervention. Pre-intervention versus post-intervention V̇O2peak (mL/kg-1/min-1) was 24.28±4.91 versus 27.06±4.82 in HIITA, 24.65±7.67 versus 27.48±8.23 in HIIT B, and 29.33±9.04 versus 33.05±9.90 in MICT. No adverse events were reported.
Conclusions: This is the first study to report the feasibility of HIIT in KTRs. Although participants struggled to achieve the required intensity (power), this study highlights the potential that exercise has to reduce cardiovascular risk in KTRs. HIIT and MICT performed on a cycle, with some modification, could be considered safe and feasible in KTRs. Larger scale trials are required to assess the efficacy of HIIT in KTRs and in particular identify the most appropriate intensities, recovery periods, and session duration. Some flexibility in delivery, such as incorporating home-based sessions, may need to be considered to improve recruitment and retention.
Trial registration: ISRCTN, ISRCTN17122775 . Registered on 30 January 2017.
Keywords: Cardiovascular disease; Chronic kidney disease; Feasibility; High-intensity interval training; Kidney transplantation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effect of high intensity interval training and moderate intensity continuous training on lymphoid, myeloid and inflammatory cells in kidney transplant recipients.Exerc Immunol Rev. 2022;28:100-115. Exerc Immunol Rev. 2022. PMID: 35452395
-
Participant acceptability of exercise in kidney disease (PACE-KD): a feasibility study protocol in renal transplant recipients.BMJ Open. 2017 Sep 24;7(9):e017494. doi: 10.1136/bmjopen-2017-017494. BMJ Open. 2017. PMID: 28947458 Free PMC article.
-
Short-term and Long-term Feasibility, Safety, and Efficacy of High-Intensity Interval Training in Cardiac Rehabilitation: The FITR Heart Study Randomized Clinical Trial.JAMA Cardiol. 2020 Dec 1;5(12):1382-1389. doi: 10.1001/jamacardio.2020.3511. JAMA Cardiol. 2020. PMID: 32876655 Free PMC article. Clinical Trial.
-
Effects of High-Intensity Interval vs. Moderate-Intensity Continuous Training on Cardiac Rehabilitation in Patients With Cardiovascular Disease: A Systematic Review and Meta-Analysis.Front Cardiovasc Med. 2022 Feb 23;9:845225. doi: 10.3389/fcvm.2022.845225. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35282360 Free PMC article.
-
Effect of High-Intensity Interval Training on Physical Health in Coronary Artery Disease Patients: A Meta-Analysis of Randomized Controlled Trials.J Cardiovasc Dev Dis. 2021 Nov 18;8(11):158. doi: 10.3390/jcdd8110158. J Cardiovasc Dev Dis. 2021. PMID: 34821711 Free PMC article. Review.
Cited by
-
The impact of high intensity training and sports on recipients of solid organ transplants: a narrative review.Front Sports Act Living. 2024 Sep 24;6:1439399. doi: 10.3389/fspor.2024.1439399. eCollection 2024. Front Sports Act Living. 2024. PMID: 39381258 Free PMC article. Review.
-
A structured, home-based exercise programme in kidney transplant recipients (ECSERT): A randomised controlled feasibility study.PLoS One. 2025 Feb 24;20(2):e0316031. doi: 10.1371/journal.pone.0316031. eCollection 2025. PLoS One. 2025. PMID: 39992959 Free PMC article. Clinical Trial.
-
Supervised vs home-based exercise program in kidney transplant recipients: A pilot pragmatic non-randomized study.World J Transplant. 2024 Dec 18;14(4):96244. doi: 10.5500/wjt.v14.i4.96244. World J Transplant. 2024. PMID: 39697462 Free PMC article.
-
Is High-Intensity Interval Training an Option for Post-Kidney Transplant Physical Rehabilitation Programmes? A Scoping Review.J Multidiscip Healthc. 2025 Feb 28;18:1231-1239. doi: 10.2147/JMDH.S491605. eCollection 2025. J Multidiscip Healthc. 2025. PMID: 40041241 Free PMC article. Review.
-
Rates of compliance and adherence to high-intensity interval training: a systematic review and Meta-analyses.Int J Behav Nutr Phys Act. 2023 Nov 21;20(1):134. doi: 10.1186/s12966-023-01535-w. Int J Behav Nutr Phys Act. 2023. PMID: 37990239 Free PMC article.
References
-
- Kiberd BA. Cardiovascular disease in kidney transplant recipients. Population. 2007;12:13.
-
- UK Renal Registry. (2021). UK Renal Registry 23rd Annual Report - data to 31/12/2019, Bristol, UK. Retrieved from renal.org/audit-research/annual-report
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
