

Multiple metastases of androgen indifferent prostate cancer in the urinary tract: two case reports and a literature review
- PMID: 35598018
- PMCID: PMC9124419
- DOI: 10.1186/s12920-022-01267-z
Multiple metastases of androgen indifferent prostate cancer in the urinary tract: two case reports and a literature review
Abstract
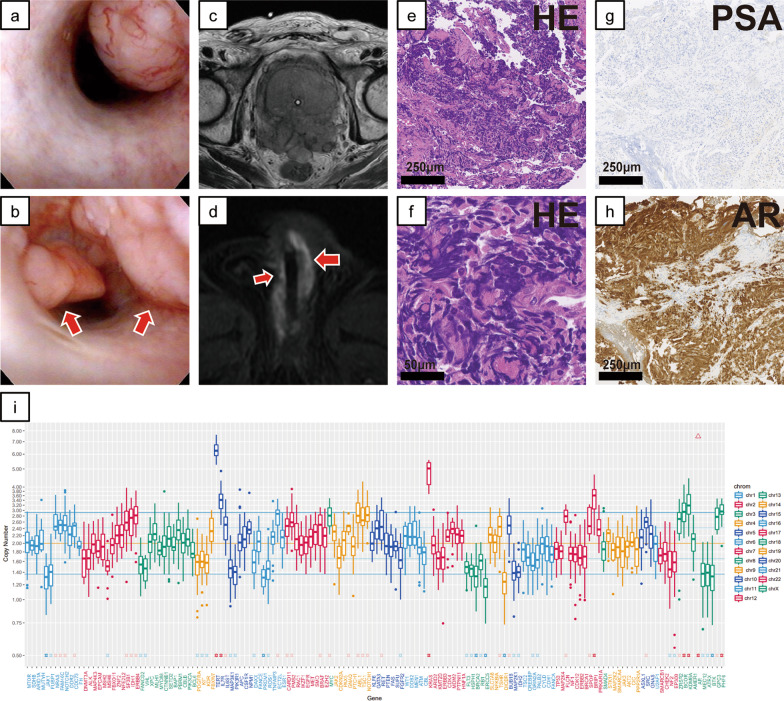
Background: Prostate cancer (PC) is mainly known to metastasize to bone, lung and liver, but isolated metastases of prostate cancer, including ductal carcinoma, in the urinary tract are very rare. We describe two patients with nodular masses in the urinary tract (the anterior urethra or the urinary bladder) that were found on cystoscopy during treatment of castration-resistant prostate cancer.
Case presentation: In both cases, the pathological diagnosis from transurethral tumor resection showed that they were androgen indifferent prostate cancer (AIPC), including aggressive variant prostate cancer (AVPC) in Case 1 and treatment-induced neuroendocrine differentiation prostate cancer (NEPC) in Case 2. In Case 1, Loss of genetic heterozygosity (LOH) of BRCA2 and gene amplification of KRAS was identified from the urethra polyps. In Case 2, homozygous deletion was observed in PTEN, and LOH without mutation was observed in RB1.
Conclusion: These are the first reports of two cases of urinary tract metastasis of AIPC.
Keywords: AR; Aggressive variant prostate cancer; BRCA2; Neuroendocrine differentiation prostate cancer; PTEN; TP53; Urinary tract metastasis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Haller B, Yao HH-I, Christidis D, Chee J, Bishop C. Clinical recurrence of prostatic ductal adenocarcinoma in the anterior urethra. J Clin Urol. 2020 doi: 10.1177/2051415820921312. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
