

Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis
- PMID: 35598608
- PMCID: PMC7613574
- DOI: 10.1016/S0140-6736(22)00478-0
Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis
Abstract
Background: Respiratory syncytial virus (RSV) is the most common cause of acute lower respiratory infection in young children. We previously estimated that in 2015, 33·1 million episodes of RSV-associated acute lower respiratory infection occurred in children aged 0-60 months, resulting in a total of 118 200 deaths worldwide. Since then, several community surveillance studies have been done to obtain a more precise estimation of RSV associated community deaths. We aimed to update RSV-associated acute lower respiratory infection morbidity and mortality at global, regional, and national levels in children aged 0-60 months for 2019, with focus on overall mortality and narrower infant age groups that are targeted by RSV prophylactics in development.
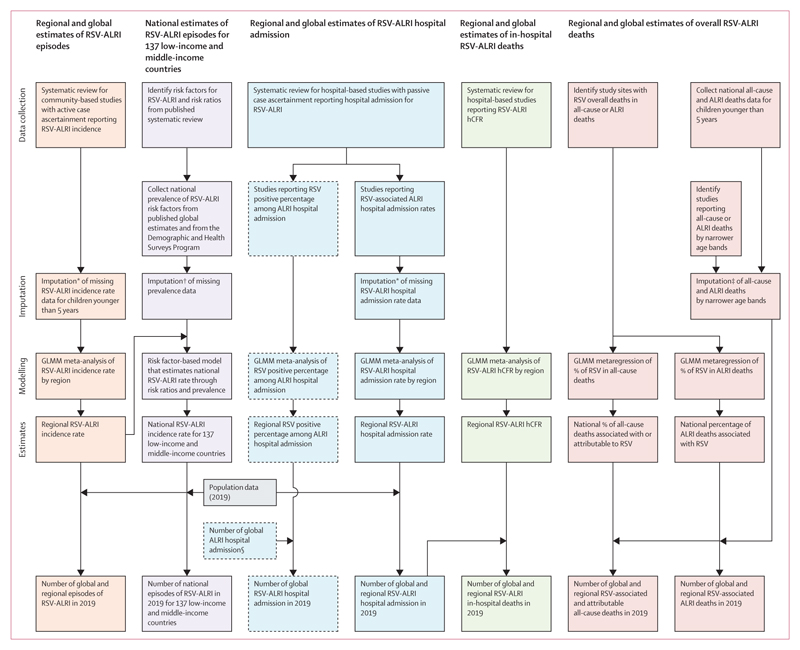
Methods: In this systematic analysis, we expanded our global RSV disease burden dataset by obtaining new data from an updated search for papers published between Jan 1, 2017, and Dec 31, 2020, from MEDLINE, Embase, Global Health, CINAHL, Web of Science, LILACS, OpenGrey, CNKI, Wanfang, and ChongqingVIP. We also included unpublished data from RSV GEN collaborators. Eligible studies reported data for children aged 0-60 months with RSV as primary infection with acute lower respiratory infection in community settings, or acute lower respiratory infection necessitating hospital admission; reported data for at least 12 consecutive months, except for in-hospital case fatality ratio (CFR) or for where RSV seasonality is well-defined; and reported incidence rate, hospital admission rate, RSV positive proportion in acute lower respiratory infection hospital admission, or in-hospital CFR. Studies were excluded if case definition was not clearly defined or not consistently applied, RSV infection was not laboratory confirmed or based on serology alone, or if the report included fewer than 50 cases of acute lower respiratory infection. We applied a generalised linear mixed-effects model (GLMM) to estimate RSV-associated acute lower respiratory infection incidence, hospital admission, and in-hospital mortality both globally and regionally (by country development status and by World Bank Income Classification) in 2019. We estimated country-level RSV-associated acute lower respiratory infection incidence through a risk-factor based model. We developed new models (through GLMM) that incorporated the latest RSV community mortality data for estimating overall RSV mortality. This review was registered in PROSPERO (CRD42021252400).
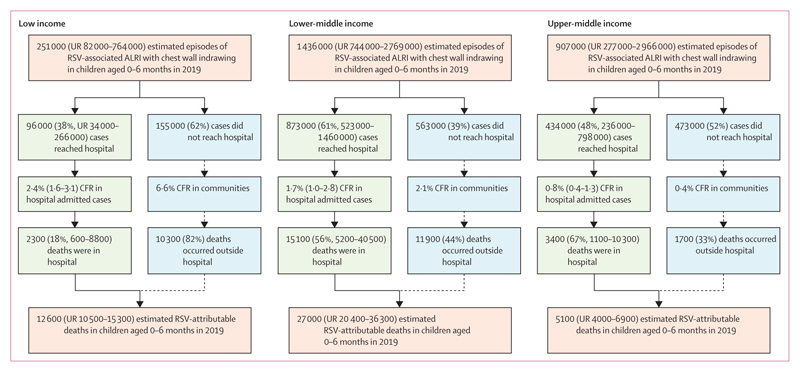
Findings: In addition to 317 studies included in our previous review, we identified and included 113 new eligible studies and unpublished data from 51 studies, for a total of 481 studies. We estimated that globally in 2019, there were 33·0 million RSV-associated acute lower respiratory infection episodes (uncertainty range [UR] 25·4-44·6 million), 3·6 million RSV-associated acute lower respiratory infection hospital admissions (2·9-4·6 million), 26 300 RSV-associated acute lower respiratory infection in-hospital deaths (15 100-49 100), and 101 400 RSV-attributable overall deaths (84 500-125 200) in children aged 0-60 months. In infants aged 0-6 months, we estimated that there were 6·6 million RSV-associated acute lower respiratory infection episodes (4·6-9·7 million), 1·4 million RSV-associated acute lower respiratory infection hospital admissions (1·0-2·0 million), 13 300 RSV-associated acute lower respiratory infection in-hospital deaths (6800-28 100), and 45 700 RSV-attributable overall deaths (38 400-55 900). 2·0% of deaths in children aged 0-60 months (UR 1·6-2·4) and 3·6% of deaths in children aged 28 days to 6 months (3·0-4·4) were attributable to RSV. More than 95% of RSV-associated acute lower respiratory infection episodes and more than 97% of RSV-attributable deaths across all age bands were in low-income and middle-income countries (LMICs).
Interpretation: RSV contributes substantially to morbidity and mortality burden globally in children aged 0-60 months, especially during the first 6 months of life and in LMICs. We highlight the striking overall mortality burden of RSV disease worldwide, with one in every 50 deaths in children aged 0-60 months and one in every 28 deaths in children aged 28 days to 6 months attributable to RSV. For every RSV-associated acute lower respiratory infection in-hospital death, we estimate approximately three more deaths attributable to RSV in the community. RSV passive immunisation programmes targeting protection during the first 6 months of life could have a substantial effect on reducing RSV disease burden, although more data are needed to understand the implications of the potential age-shifts in peak RSV burden to older age when these are implemented.
Funding: EU Innovative Medicines Initiative Respiratory Syncytial Virus Consortium in Europe (RESCEU).
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
YL reports grants from Wellcome Trust and WHO outside the submitted work. MTC reports grants from the Bill & Melinda Gates Foundation related to the submitted work, grants from MITS Surveillance Alliance, and support for attending the RSVVW meeting from ReSViNET outside the submitted work. SAM reports grants from Pfizer, Minervax, GSK, the Gates Foundation, and South African Medical Research Council; honoraria from the Gates Foundation; and participation on data safety monitoring boards for PATH and CAPRISA, outside the submitted work. SBO reports grants from the Gates Foundation outside the submitted work. EAFS reports grants, personal fees, and travel fees from AstraZeneca, Merck, Regeneron, Pfizer, and Roche; consultation, lecture fees, travel support, and data and safety monitoring board fees from AbbVie; data and safety monitoring board fees from GSK; consultation fees from Alere; grants from Johnson & Johnson; and grants and travel support from Novavax outside the submitted work. HC reports grants from the Gates Foundation outside the submitted work. AGo reports grants from the National Institute of Allergy and Infectious Diseases and Centers for Disease Control and Prevention (CDC) related to the submitted work and participation on an advisory board for Janssen outside the submitted work. TH reports personal fees from Janssen and Sanofi Pasteur outside the submitted work. AK reports grants from CDC and honoraria from CDC and WHO outside the submitted work. AM-I reports grants from FISABIO-Public Health, Sanofi Pasteur, and CIBER-ESP (ISCIII) related to the submitted work, honoraria from MSD as a speaker in a vaccine research course, and travel grants for attending meetings sponsored by Sanofi, outside the submitted work. HCM reports grants from National Health and Medical Research Council related to the submitted work and honoraria from MSD for participation on an expert input forum outside the submitted work. DJN reports grants from Wellcome Trust related to the submitted work. EO reports receipt of PhD scholarship from DAAD (German Academic Exchange Service) Government of Ghana scholarship outside the submitted work. CR reports grants from CDC in collaboration with US Naval Medical Research Unit No6 related to the submitted work and grants from South America Influenza Initiative outside the submitted work. AS reports grants from University of Colorado outside the submitted work. RS reports grants from Merck outside the submitted work. SKS reports salaries from GSK for working on the data abstraction, leading the prospective cohort study from which the data were abstracted, and for providing input for the manuscript development related to the submitted work and stock in GSK outside the submitted work. AvG reports grants from CDC outside the submitted work. DW reports grants from Murdoch Children’s Research Institute related to the submitted work and honoraria from MSD for participation on an expert input forum outside the submitted work. L-MY reports grants from Japan Agency for Medical Research and Development related to the submitted work and honoraria for a lecture from MSD KK. HJZ reports grants from the Gates Foundation, South African Medical Research Council, National Institutes for Health, and AstraZeneca and participation on WHO Technical Advisory Group with no payment, outside the submitted work. HN reports grants from the Innovative Medicines Initiative related to the submitted work and consulting fees from the Gates Foundation, Pfizer, and Sanofi; honoraria from AbbVie; support from Sanofi for attending meetings; and participation on advisory boards from Sanofi, Janssen, Novavax, Reviral, Resvinet, and WHO outside the submitted work.
Figures
Comment in
-
Need for improved global measurement of early childhood respiratory syncytial virus disease.Lancet. 2022 May 28;399(10340):1993-1995. doi: 10.1016/S0140-6736(22)00623-7. Epub 2022 May 19. Lancet. 2022. PMID: 35598609 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
