

The role of re-resection in recurrent hepatocellular carcinoma
- PMID: 35599252
- PMCID: PMC9468093
- DOI: 10.1007/s00423-022-02545-1
The role of re-resection in recurrent hepatocellular carcinoma
Abstract
Purpose: While liver resection is a well-established treatment for primary HCC, surgical treatment for recurrent HCC (rHCC) remains the topic of an ongoing debate. Thus, we investigated perioperative and long-term outcome in patients undergoing re-resection for rHCC in comparative analysis to patients with primary HCC treated by resection.
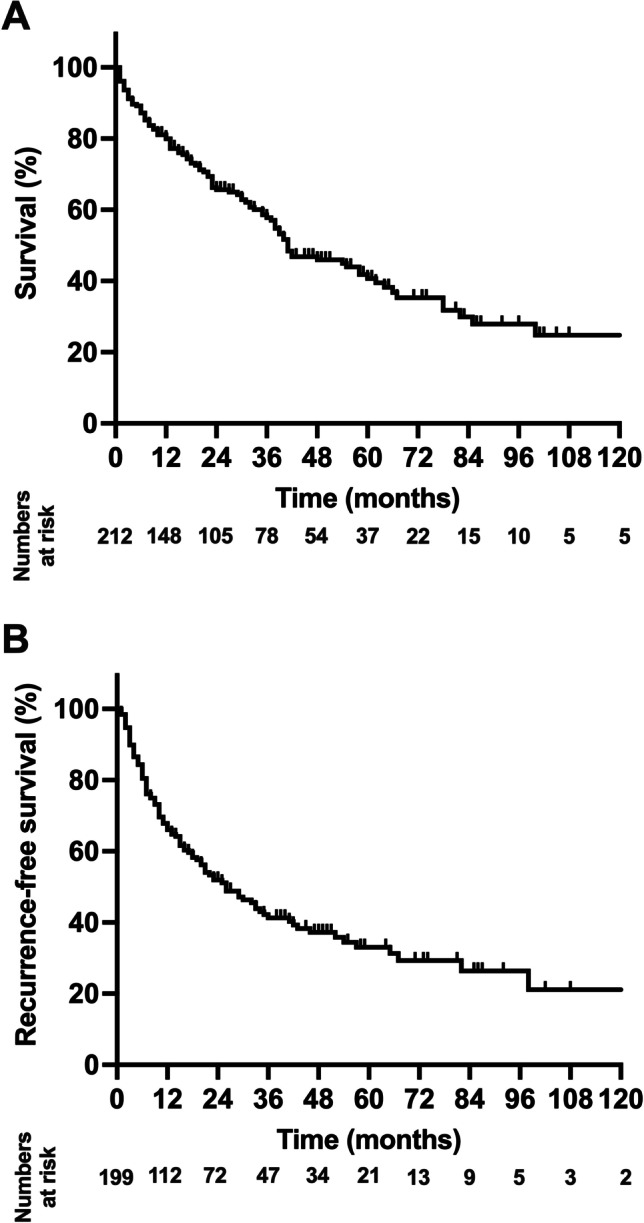
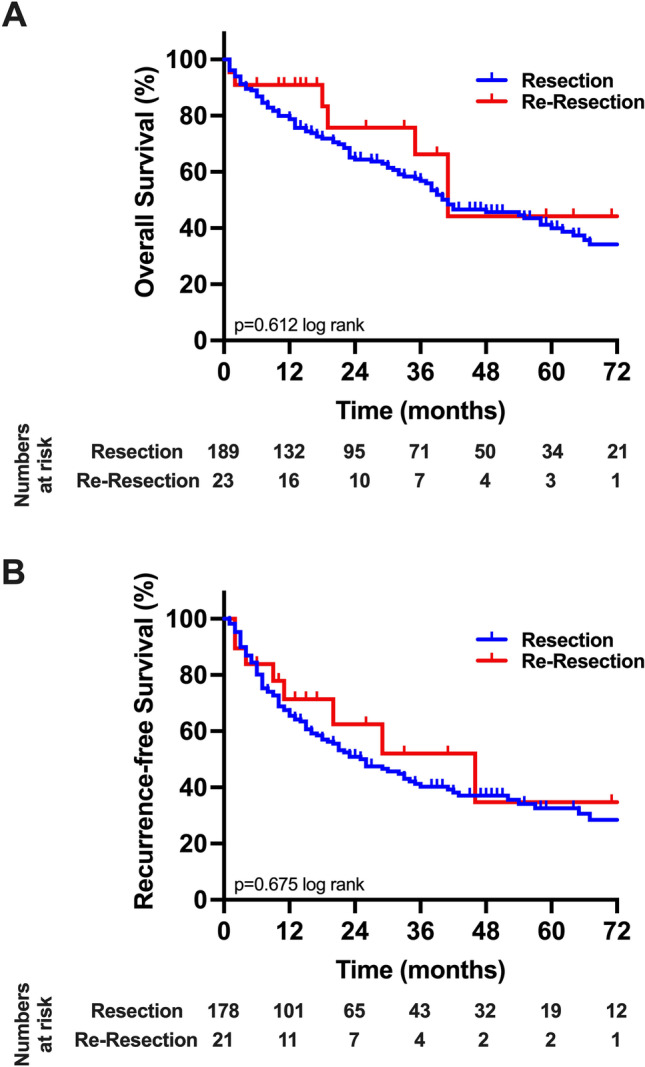
Methods: A monocentric cohort of 212 patients undergoing curative-intent liver resection for HCC between 2010 and 2020 in a large German hepatobiliary center were eligible for analysis. Patients with primary HCC (n = 189) were compared to individuals with rHCC (n = 23) regarding perioperative results by statistical group comparisons and oncological outcome using Kaplan-Meier analysis.
Results: Comparative analysis showed no statistical difference between the resection and re-resection group in terms of age (p = 0.204), gender (p = 0.180), ASA category (p = 0.346) as well as main preoperative tumor characteristics, liver function parameters, operative variables, and postoperative complications (p = 0.851). The perioperative morbidity (Clavien-Dindo ≥ 3a) and mortality were 21.7% (5/23) and 8.7% (2/23) in rHCC, while 25.4% (48/189) and 5.8% (11/189) in primary HCC, respectively (p = 0.851). The median overall survival (OS) and recurrence-free survival (RFS) in the resection group were 40 months and 26 months, while median OS and RFS were 41 months and 29 months in the re-resection group, respectively (p = 0.933; p = 0.607; log rank).
Conclusion: Re-resection is technically feasible and safe in patients with rHCC. Further, comparative analysis displayed similar oncological outcome in patients with primary and rHCC treated by liver resection. Re-resection should therefore be considered in European patients diagnosed with rHCC.
Keywords: HCC; Re-resection; Surgery; Tumor recurrence.
© 2022. The Author(s).
Conflict of interest statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was conducted at the UH-RWTH in accordance with the requirements of the Institutional Review Board of the RWTH-Aachen University (EK EK 503/21). All authors declare no conflict of interest.
The authors declare no competing interests.
Figures
References
-
- Lurje G, Bednarsch J, Czigany Z, Amygdalos I, Meister F, Schoning W, Ulmer TF, Foerster M, Dejong C, Neumann UP. Prognostic factors of disease-free and overall survival in patients with hepatocellular carcinoma undergoing partial hepatectomy in curative intent. Langenbeck's archives of surgery/Deutsche Gesellschaft fur Chirurgie. 2018;403(7):851–861. doi: 10.1007/s00423-018-1715-9. - DOI - PubMed
-
- Vitale A, Burra P, Frigo AC, Trevisani F, Farinati F, Spolverato G, Volk M, Giannini EG, Ciccarese F, Piscaglia F, Rapaccini GL, Di Marco M, Caturelli E, Zoli M, Borzio F, Cabibbo G, Felder M, Gasbarrini A, Sacco R, Foschi FG, Missale G, Morisco F, Svegliati Baroni G, Virdone R, Cillo U, Cancer IL, g, Survival benefit of liver resection for patients with hepatocellular carcinoma across different Barcelona Clinic Liver Cancer stages: a multicentre study. J Hepatol. 2015;62(3):617–624. doi: 10.1016/j.jhep.2014.10.037. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
