

Efficacy of thoracotomy and thoracoscopic-assisted esophageal surgery in conversion and salvage surgeries: a retrospective study
- PMID: 35599328
- PMCID: PMC9125810
- DOI: 10.1186/s12957-022-02637-8
Efficacy of thoracotomy and thoracoscopic-assisted esophageal surgery in conversion and salvage surgeries: a retrospective study
Abstract
Background: The esophagus has no serosa; therefore, esophageal cancer may quickly invade its adjacent organs. In recent years, reports of conversion surgery (CS) and salvage surgery (SS) have described resection of esophageal cancer previously considered unresectable, with the addition of intensive preoperative chemotherapy or chemoradiotherapy. Currently, there is no established method for determining whether tumor excision is possible. Additionally, differences in surgical approaches between facilities may influence outcome after resection. However, the option for resection is considered a significant factor in determining a patient's prognosis.
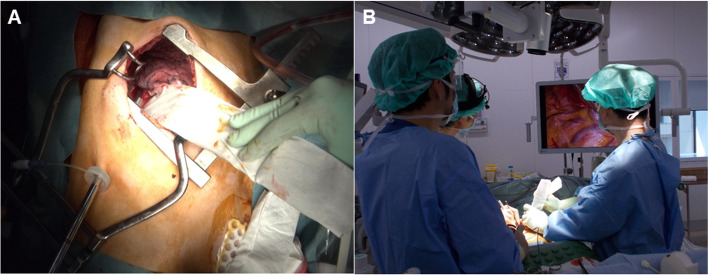
Methods: Patients who were diagnosed with advanced-stage (T3 or higher) squamous cell carcinoma of the esophagus and subsequently underwent resection with CS or SS were included in the study. Resection was performed through a small thoracotomy using a thoracoscope. Clinicopathologic factors, such as complete resection rate (R0) and prognosis, were investigated.
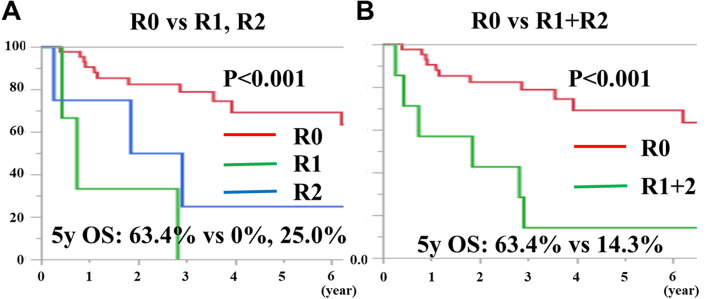
Results: A total of 49 surgeries were conducted: 39 CS and 10 SS cases. The male-to-female ratio was 37:12. R0:R1:R2 equals 42:3:4, and the R0 resection rate was 85.7%. The 5-year survival rates for CS and SS cases were 69.2% and 32.1%, respectively. The 5-year survival rates for R0, R1, and R2 resections were 63.4%, 0.0%, and 25.0%, and those for R0 and R1 + 2 resections were 63.4% and 14.3%, respectively, indicating that the prognosis for R0 resection cases was significantly better (P = 0.001 and P = 0.001, respectively). Regarding chemotherapy for CS, 29 patients received 5-FU and cisplatin therapy, whereas 10 patients received 5-FU, cisplatin, and docetaxel (DCF) therapy. After 2015, the ratio of DCF was significantly high, and the R0 resection rate was 100% in patients who received DCF therapy.
Conclusions: In this study, a satisfactory R0 rate was achieved using the magnifying effect of the thoracoscope while ensuring safety during thoracotomy.
Trial registration: This was a single-center cohort study wherein clinical data were retrospectively registered. This study was approved by the Chiba Cancer Center review board (H29-262). All procedures adhered to the ethical standards of the responsible committee on human experimentation and the Helsinki Declaration of 1964 and its later amendments.
Keywords: Chemoradiotherapy; Chemotherapy; Conversion surgery; Esophageal cancer; Salvage therapy.
© 2022. The Author(s).
Conflict of interest statement
Not applicable.
Figures



References
-
- Rustgi A, El-Serag HB. Esophageal carcinoma. N Engl J Med. 2015;372:1472–1473. - PubMed
-
- Yokota T, Kato K, Hamamoto Y, Tsubosa Y, Ogawa H, Ito Y, et al. A 3-year overall survival update from a phase 2 study of chemoselection with DCF and subsequent conversion surgery for locally advanced unresectable esophageal cancer. Ann Surg Oncol. 2020;27:460–467. doi: 10.1245/s10434-019-07654-8. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
