

The end of life of patients with COVID-19 in intensive care unit and the stress level on their family members: A cross-sectional study
- PMID: 35599352
- PMCID: PMC9348431
- DOI: 10.1111/nicc.12783
The end of life of patients with COVID-19 in intensive care unit and the stress level on their family members: A cross-sectional study
Abstract
Background: During the Coronavirus disease 2019 (COVID-19) pandemic, hospital visits were suspended and video calls were offered to connect patients with their family members, especially toward the end of life (EoL).
Aim: The primary aim was to describe EoL care for COVID-19 patients dying in an intensive care unit (ICU). The secondary aim was to explore whether making video calls and allowing visits was associated with lower death-related stress in family members.
Design: Single centre cross-sectional study. The setting was the ICU of a COVID-19 center in northern Italy, during the first year of the pandemic. Data on patients who died in the ICU were collected; death-related stress on their family members was measured using the Impact of Event Scale-Revised (IES-R). The statistical association was tested by means of logistic regression.
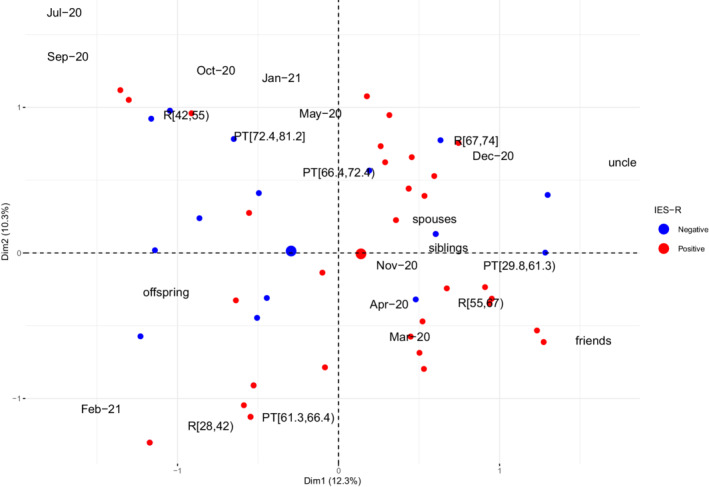
Results: The study sample included 70 patients and 56 family members. All patients died with mechanical ventilation, hydration, nutrition, analgesia and sedation ongoing. Resuscitation procedures were performed in 5/70 patients (7.1%). Only 6/56 (10.7%) of the family members interviewed had visited their loved ones in the ICU and 28/56 (50%) had made a video call. EoL video calls were judged useful by 53/56 family members (94.6%) but all (56/56, 100%) wished they could have visited the patient. High-stress levels were found in 38/56 family members (67.9%), regardless of whether they were allowed ICU access or made a video call. Compared with other degrees of kinship, patients' offspring were less likely to show a positive IES-R score (odds ratio [OR] 0.22, 95% confidence interval [CI] 0.05 to 0.89).
Conclusions: During the first year of the COVID-19 pandemic, patients died without their family members at the bedside while on life-sustaining treatment. Stress levels were high in most family members, especially in patients' spouses. Video calls or ICU visits were judged favourably by family members but insufficient to alleviate death-related stress.
Relevance for clinical practice: During a pandemic, ICU access by patients' family members should be considered, particularly as the time of death approaches. Although generally appreciated by family members, EoL video calls should be arranged together with other measures to alleviate death-related stress, especially for the patient's spouse.
Keywords: COVID-19; critical care; end-of-life care; stress; visitors to patients.
© 2022 The Authors. Nursing in Critical Care published by John Wiley & Sons Ltd on behalf of British Association of Critical Care Nurses.
Figures
References
-
- WHO Coronavirus (COVID‐19) Dashboard, https://covid19.who.int/ (accessed February 15, 2022).
-
- Kleinpell R, Heyland DK, Lipman J, et al. Patient and family engagement in the ICU: report from the task force of the world Federation of Societies of intensive and critical care medicine. J Crit Care. 2018;48:251‐256. - PubMed
-
- Davidson JE, Aslakson RA, Long AC, et al. Guidelines for family‐centered Care in the Neonatal, pediatric, and adult ICU. Crit Care Med. 2017;45:103‐128. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
